- Open access
- Published: 26 August 2024

Identification of mothers with mental health problems is accidental: perceptions of health care providers on availability, access, and support for maternal mental health care for adolescent mothers in Malawi
- Chimwemwe Tembo 1 ,
- Linda Portsmouth 2 &
- Sharyn Burns 2
BMC Health Services Research volume 24 , Article number: 983 ( 2024 ) Cite this article
144 Accesses
Metrics details
Integration of maternal mental health into primary health care is considered a strategy to improve access to mental health support in low- and middle-income countries (LMICs). Health care workers’ (HCWs) and traditional practitioners’ (traditional healers, herbalists, traditional birth attendants, spiritual healers, prophets, and community health volunteers) perceptions of the availability and management of adolescent mothers’ maternal mental health care were explored in rural Malawi. Recognizing and identifying the barriers associated with access to maternal mental health support is essential to improving the mental health of adolescent mothers.
A descriptive qualitative design (DQ) was used to explore HCWs’ and traditional practitioners’ perceptions of maternal mental health services for adolescent mothers. In-depth interviews were conducted with HCWs ( n = 6), and three focus group discussions were conducted with 30 community-based traditional practitioners. Participants were purposefully recruited because they provide formal or informal health services to adolescent mothers during the postnatal period at Mitundu Rural Hospital and its catchment area in Lilongwe District, in Malawi. Interviews were analyzed using reflective thematic analysis and inductive thinking.
Thematic analysis found four themes to describe access to maternal mental health care for adolescent mothers. Participant perceptions were themed around health system challenges and how cultural background and beliefs influence access to mental health care and support. The themes were: (1) Inadequate staff development; (2) Limited resources (medication and infrastructure); (3) Limited policy and guidelines implementation; and (4) Cultural background and belief influence on help-seeking. HCWs suggested improving pre-service and in-service training to improve mental health assessment of mothers, while traditional practitioners wanted to increase their awareness of mental health issues.
Participants emphasized that multifaceted factors influenced access to mental health support. These factors affect the assessment, treatment, and support of adolescent mothers and help-seeking by mothers. Therefore, strengthening the healthcare system and empowering providers with the knowledge and skills to recognize at-risk mothers and provide timely support is essential.
Peer Review reports
The burden of poor maternal mental health in adolescent mothers is a public health concern [ 1 ]. Worldwide, about 10% of pregnant women and 13% of those that have given birth, experience some mental disorder [ 2 ]. The prevalence rates of CMDs among perinatal women are two to three times more prevalent in Low to Middle-Income Countries (LMIC) compared to High-Income Countries (HIC) [ 1 , 2 ]. Studies in LMIC reported a prevalence rate of 19.8% after childbirth [ 2 ]. In sub-Saharan Africa (SSA), the prevalence rates of CMDs range from 10 to 39% postnatally [ 1 , 3 ]. In Malawi, the prevalence of depressive disorders during the perinatal period ranges from 21 − 42% [ 4 , 5 ]. A recent study in Malawi found a prevalence of postnatal depression of 43.2% among adolescent mothers [ 6 ]. Motherhood initiated during adolescence can have its own challenges, hence the urgent need for early identification and treatment of mental health problems. Adolescence brings various challenges and vulnerabilities associated with physical, cognitive, and psychological well-being [ 7 , 8 ]. For adolescent mothers, this period can be more challenging and may complicate social roles [ 9 , 10 ]. Considering the broad implications of adolescent motherhood on the well-being of the mother and their child’s development, early identification and effective treatment are essential for preventing the escalation of mental health problems [ 11 ]. Untreated maternal mental health is the largest contributor to the disease burden for women of childbearing age [ 12 ]. Furthermore, adolescent mothers with untreated postnatal mental health problems are more likely to have low birth weight, poor interactions with their babies, neonatal complications that affect breastfeeding, baby care, parenting and babies may develop malnutrition and frequent hospitalisation [ 13 , 14 ].
Further, access to healthcare is critical to the performance of healthcare systems globally [ 15 ]. However, some challenges exist in LMICs for people with specific health conditions regarding access to comprehensive care [ 16 ]. For example, less than half of affected mothers with mental health conditions have access to adequate treatment and healthcare [ 16 ]. Mental health care access refers to the opportunity to have mental health care needs fulfilled by having access to appropriate and culturally secure mental health services and/or when communities can use appropriate mental health services in proportion to their needs [ 15 ]. The disparity between the number of individuals experiencing mental health issues and the number who receive appropriate treatment is referred to as the treatment gap. In many LMICs, this gap is estimated to be between 75% and 80% [ 17 ].
The Government of Malawi is committed to improving health and wellbeing in line with the WHO recommendations and Sustainable Development Goals (SDG) three and five. The Malawian Ministry of Health has developed a mental health policy that aims to provide comprehensive and accessible mental health care services to all citizens of Malawi, including the mental health care needs of special groups [ 18 , 19 , 20 ]. However, the implementation of the policy is limited, particularly in managing maternal mental health [ 18 ]. The challenges to accessing mental health care in SSA countries and other LMICs derive from inadequate mental health support from the health system [ 18 ], economic hardships, a negative societal perception of adolescent motherhood, rural residency, and mothers’ low education levels [ 12 , 18 , 21 , 22 , 23 ]. Additionally, various cultural factors, such as polygamy and traditional practices around gender roles and marriage, impact access to mental health care [ 24 , 25 ]. Furthermore, adolescent mothers in SSA have lower levels of help-seeking behaviours [ 24 ], which has been linked to a perceived lack of confidentiality, negative healthcare worker attitudes, and a lack of services tailored to their unique needs [ 16 ]. For example, research with HIV-positive adolescent mothers aged 15–19 years in Malawi exploring barriers and facilitators of prevention of mother-to-child transmission of HIV found adolescent mothers expressed a preference for peer-led, age-appropriate, non-judgmental maternal health support services that link communities and facilities to pragmatically address barriers of stigma, and health system complexity [ 14 ]. The Malawian study highlighted the need for tailored services that consider the specific needs of adolescent and young mothers.
Access to healthcare is critical in the management of postnatal depression, and the role of health workers in the prevention of maternal mental health cannot be underestimated [ 26 ]. A Malawian study [ 6 ] found that adolescent mothers who interacted with a health worker during the postnatal period were less likely to report depression than their peers who did not experience any health worker contact. Interaction with a health worker may provide an opportunity for mental health screening and subsequent referral and support [ 26 ]. Perinatal screening is considered an important strategy for the early detection of mental health problems across different healthcare settings and within different economic settings [ 21 , 24 , 27 ]. Furthermore, studies from some LMICs found that perinatal women accepted screening for common mental disorders as part of their primary care [ 28 , 29 ]. However, there are challenges in implementing screening in some LMICs due to a lack of knowledge among health workers around screening for mental health issues, staff workload, the lack of clinical guidelines for the screening of pregnant and parenting teens, and limited specialized mental health services [ 18 , 26 , 30 ]. Understanding barriers and facilitators to help-seeking is fundamental for developing contextual interventions, enhancing prevention, improving identification, and prompting appropriate treatment [ 11 ].
In Malawi, the use of traditional healing is widespread [ 31 ], unlike in HIC, where women are more likely to seek help from biomedically trained doctors and midwives [ 32 ]. One Malawian study found that the prevalence of people with mental disorders who seek the services of traditional healers before visiting a hospital was 22.7% [ 33 ]. Furthermore, another Malawian study found the prevalence of herbal medicine use among all women during pregnancy was estimated at 25.7% in 2018 with use of herbal medicine decreasing among older mothers, with younger women being more likely to use herbal medicine [ 31 ]. Another study in Zimbabwe found the use of herbal medicine was more common among women during their first pregnancy or first childbirth [ 34 ]. In the context of Malawi, traditional healers provide an alternative or additional approach to mental health care [ 33 ]. Therefore, they are key providers in the health care system in Malawi and many other SSA countries [ 14 , 32 , 34 , 35 ]. Further, the ethnobotanical research on the traditional use of plants for improving healthcare has been based on knowledge held by traditional practitioners [ 14 , 35 ]. A study in Mali found that traditional practitioners have broad experience and knowledge about the herbal treatment of pregnant ailments [ 35 ]. Understanding mothers’ use of traditional healers can help identify opportunities to address existing access to health services challenges, thereby improving maternal mental health outcomes [ 31 ].
The World Health Organization (WHO) recommends the incorporation of mental health prevention, early intervention, and promotion strategies in maternal and child health services to identify at-risk mothers early, therefore reducing the morbidity and mortality associated with poor mental health [ 36 ]. Community-based health workers are important in supporting people with their health because they are local, trusted by communities, and integrated within the health system [ 37 ]. This study explored the perceptions of healthcare workers (HCWs) and traditional practitioners regarding the access to maternal mental health care by adolescent mothers in rural Malawi.
The public health care system in Malawi adopts a three-tier health care delivery system based on three levels of health care: primary, secondary, and tertiary [ 38 , 39 ]. The healthcare system comprises central hospitals, district hospitals, health centers, community hospitals, clinics, and rural hospitals. Each district hospital serves an average population of 600,000 to 900,000 within a geographical distance of 15 to 20 km. District hospitals manage smaller rural hospitals, health centers and health posts [ 38 ]. There are twenty-eight administrative districts and twenty-six district hospitals in Malawi (The Malawi Government, 2005). District and rural hospitals operate 24 h, 7 days per week. This study was conducted at Mitundu, located about 40 km east of Lilongwe, the capital city of Malawi. Mitundu is a rural area that has a population of 147,823 [ 38 ]. Mitundu Rural Hospital (MRH), the only health facility in the area, was chosen because it serves a relatively higher number of people compared to other facilities within Lilongwe District, with an average of 135 deliveries by adolescent mothers every month. The area has more cases of adolescent marriages compared to urban areas [ 6 ]. The hospital also operates thirteen outreach clinics, which are visited monthly by community health workers. MRH provides free outpatient, maternal and child health, family planning and maternity services. The reproductive health services offered at district hospitals include antenatal care, labor and delivery, postnatal care, family planning, cancer screening, and the management of sexually transmitted infections. The facility has forty-six clinical health workers, with eight working in maternal and child health services. Saint John of God Hospitaller Services, Malawi, supports mental health services through conducting monthly outpatient clinics for people with mental illnesses.
Study design and participants
A qualitative-descriptive design was used to explore the views of HCWs and traditional practitioners’ perceptions of maternal mental health services for adolescent mothers. The HCWs comprised medical practitioners (doctors) and nurses employed in the Maternal and Child Health Department (MCH) at the MRH. Traditional practitioners comprised traditional healers, herbalists, traditional birth attendants, spiritual healers, prophets, and community health volunteers. Community health volunteers are lay community members who liaise with HCWs to assist with health promotion activities in the community.
In-depth interviews were conducted with HCWs to explore their perspectives, experiences and attitudes around their understanding and knowledge of healthcare services and how they are available and accessible. HCWs working in the Maternal and Child Care Department (MCH) were selected as they were in a position to provide a rich insight into appropriate and equitable intervention programs that would meet the needs of postnatal mothers [ 40 ]. In-depth interviews allowed participants to share their understanding in a non-threatening environment [ 40 ]. Interviews enabled the collection of rich and deep contextual data that could reveal underlying reasons behind delivering maternal mental health services, considering the small number of potential participants [ 40 ]. In addition, due to a limited number of HCWs and the need to schedule data collection around work rosters, interviews were deemed the most effective method to collect data from this group.
Traditional practitioners participated in focus group discussions (FGDs), which enabled the discussion of local knowledge and drew on the complex personal experiences, beliefs, perceptions, and attitudes of participants about adolescents’ mental health through moderated interaction [ 41 , 42 ]. FGDs were employed to gain a greater understanding of traditional practitioners’ role in providing mental health care services [ 43 ]. These discussions were used to gather diverse views from multiple participants and allowed for robust discussion [ 42 ]. Our study was reported according to the consolidated criteria for reporting qualitative studies COREQ [ 44 ] (Supplementary file 3).
A purposive sampling method [ 45 , 46 ] was used to recruit HCWs who worked in the maternal and child health departments at MRH. The in-depth interviews included six HCWs: two medical doctors, two community nurses, and two registered nurse midwives. All HCWs employed in the Department of Maternal and Child Health at MRH during the data collection period were invited and consented to participate. These HCWs were purposively invited to participate because they are consistently in contact with perinatal mothers during their provision of maternal and child health services [ 26 ]. Traditional practitioners were purposively invited to participate in FGDs to achieve variation in gender and the type of services they provide. Thirty traditional practitioners participated in three FGDs and were grouped according to their roles to ensure that participant groups were relatively homogenous. The three FGDs were conducted with traditional healers (six males and four females), community volunteers (eight females and two males), and spiritual healers (three females and one male prophet and six female traditional birth attendants who also use spiritual healing).
Recruitment of participants and procedures
This study was approved by the Curtin University Human Research Ethics Committee (HRE2021-0223) and the Malawian Ethics Board National Committee on Research Ethics in the Social Sciences and Humanities (P.05/21/575). HCWs were recruited at MRH in their designated work departments. An appointment was scheduled within the hospital at a convenient place and time for each HCW. HCWs were provided with an English version of the information sheet describing the research and procedures and provided consent prior to participating.
Traditional practitioners were recruited through a community health worker who lived within the Mitundu catchment area. An appointment was scheduled to meet potential participants at a convenient community shelter. All participants received information about the study, which was read in Chichewa by the researcher prior to each FGD, and consent was provided prior to participating.
Data collection
Interview guides were used to guide data collection for individual face-to-face semi-structured interviews and FGDs (supplementary files 1 and 2). The interview guides were tested with two HCWs who were not participating in the study to develop the lines of questioning when probing and ensure any ambiguities were excluded and clarified before initiating data collection. Open questions to elicit free responses were used. Questions focused on understanding mental health challenges faced by adolescent mothers during the postnatal period (Fig. 1 ). The opening questions for HCWs and traditional practitioners explored participants’ understanding of the common mental health problems and disorders that affect adolescent mothers during the postpartum period, with some probing questions to explore further understanding of how common these mental health problems are in the catchment area. Participants were also asked about how they identify and manage adolescent mothers who have mental health problems (supplementary files 1 and 2). The first author conducted all in-depth interviews with HCWs and two of the FGDs. One FGD was facilitated by a research assistant (CN).

Model describing HCW and traditional healers’ perceptions of availability, access and support for adolescent mothers
Data collection took place between September 2021 and March 2022. Individual interviews were carried out by CT, PK, and CN (Malawian mental health practitioners and researchers fluent in Chichewa and English). The FGD discussions were moderated by CT and CN while PK took notes. The interviews and FGDs were conducted face-to-face, recorded on a digital recorder, and transcribed verbatim. After each interview, member validation was conducted to ensure participant perspectives and experiences were accurately represented. Interviews with HCWs were conducted in English. All FGDs were conducted in Chichewa. Interviews lasted an average of 30 min to an hour, and FGDs lasted 45 min to an hour. Field notes and a reflexive diary that included non-verbal communication and observations were recorded to supplement recorded data.
Prior experiences, assumptions, and beliefs can inevitably impact the data collection [ 47 ]. The lead researcher in this study (CT) drew upon her background as someone who experienced adolescent motherhood and is now a mental health nurse in her mid-forties. This experience informed the researcher’s understanding of participants’ perspectives, attitudes, and experiences regarding motherhood. Therefore, the researcher implemented self-reflection and awareness to ensure bracketing. The researcher kept a reflexive diary throughout the data collection process, recording thoughts, emotions, and observations while engaging with participants and gathering data. This served as a resource for analyzing the positionality and potential biases. Additionally, the researcher collaborated with participants to collectively construct shared realities. The construction of reality is a collaborative process between the researcher and the topic under investigation, influenced by the subjective experiences of everyone involved [ 48 ]. However, the researcher minimized biased approaches during data collection by holding a neutral stance and not sharing her experiences and views while prompting and guiding the discussions. The aforementioned statements pertain to epistemological presuppositions regarding acquiring knowledge about reality [ 47 ].
De-identified transcripts were organised using NVivo version 10 [ 49 ] and analysed using thematic analysis [ 50 , 51 ]. The study employed Braun and Clarke [ 51 ] six-phases of reflexive thematic analysis: (1) familiarization with the data; (2) generating initial codes; (3) generating themes; (4) reviewing the themes; (5) final review and defining of themes; and (6) writing the results. During this process, the data was familiarized by reading and re-reading the transcripts and interview notes and noting ideas. Then, using open coding, transcripts were initially coded by (CT) and (MZ) to generate initial codes using an inductive and data-driven approach. CT and MZ coded separately during this process and then discussed the coding. Themes were generated according to the patterns of codes identified, which were grouped and allocated to a theme. The themes were discussed and confirmed by authors SB, CT, and LP to ensure the themes aligned with the coded extracts. Ongoing analysis enabled the refinement of the specifics of each theme and the generation of clear definitions and names of themes and subthemes [ 50 , 52 , 53 ]. The final step was the write-up of the results. Constant comparison by the research team achieved confirmability and dependability. The supervisory team (SB and LP) contributed to the data interpretation and ongoing reviews of the results [ 54 ]. The involvement of a team helped remove potential bias and strengthen the results [ 44 ].
Healthcare providers (HCPs) views regarding the availability, accessibility, and management of maternal mental health of adolescent mothers were explored. Participants ( n = 36) included six HCWs who participated in in-depth individual interviews and 30 traditional practitioners, including 10 traditional healers, 10 community volunteers, six traditional birth attendants and four spiritual healers who participated in the three FGDs (9 males and 21 females). Eighteen participants were Christians, four were Muslims, and eight belonged to traditional religions. Ten participants had never been to school.
Overview of themes and conceptual model
Four main themes emerged to help understand the perceptions of healthcare workers (HCWs) and traditional practitioners regarding the access and availability of mental health services for adolescent mothers in rural Malawi. The themes of inadequate staff development , limited resources , limited policy , and guidelines implementation pertain to health systems. The theme C ultural background and beliefs influencing seeking help describes cultural norms.
Inadequate staff development
The theme of inadequate staff development has four subthemes: health providers’ skills and knowledge , standard mental health screening tools , qualified mental health professionals , and health worker workforce.
Health provider’s skills and knowledge
All healthcare providers acknowledged encountering many adolescent mothers during their daily activities. HCWs reported focusing on physical examinations, nutrition assessments, nutrition counselling sessions and other health education sessions for pregnant mothers in clinics and at the community level. However, they did not address mental health. However, HCWs perceived themselves to be strategically positioned to provide initial mental health assessments and support to mothers. Some HCWs acknowledged their hesitancy to include mental health assessments as they felt they lacked the skills to identify symptoms of mental health problems and to provide appropriate mental health support. Furthermore, they expressed a need for regular professional development, for example:
Some of health workers have the skills but… most of us do not have the skills to conduct a mental health assessment…. An in-service or reorientation would be good. Of course , we had a training during our clinical placement but…. psychiatric or mental health is difficult , we have forgotten (HCW1) .
Similarly, traditional practitioners also expressed concerns about their limited awareness about mental health and perceived deficiencies in counselling skills. Community volunteers and traditional birth attendants do not routinely include mental health care. Many community volunteers had received prior training in conducting home visits to pregnant women, offering nutrition education, and performing basic physical assessments, which they believed positioned them well to support mothers in crisis before directing them to clinics. While traditional practitioners discussed their need for basic counselling skills, they also recognized the need for experienced counsellors they could refer adolescent mothers to. Other traditional practitioners, such as traditional birth attendants and herbalists, also felt they would benefit from mental health awareness and basic counselling skills.
The major reason for us who live and work in the community…. We do not have the capacity or basic skills for counselling or communicating with someone about their mental health. We do not have the knowledge for counseling. We need counsellors…. To be honest we don’t teach about mental health but about nutrition only because we don’t have the required skills or knowledge in the mental health field. (Community volunteer FDG1)
If there was an opportunity for us to learn how to manage mental health and teach about mental health , (it would) be good …. so that we can help adolescent mothers live without stress. We will be incredibly grateful also because we will add more knowledge to what we already teach mothers . ( Community volunteer FDG1).
Standard mental health screening tools
Most HCWs were willing to screen women for possible common mental health problems. However, they attributed the lack of culturally approved screening instruments as a challenge to screening. HCWs felt it important to have a standard screening tool for common disorders incorporated into their routine assessment guides. They reported that most adolescent mothers with common mental health issues requiring help go unrecognized, especially when they look happy or do not show any visible signs of sadness. One health worker summarized this sentiment, suggesting the identification of mothers with mental health problems is mostly “accidental’ due to the lack of formal screening and assessment.
Most of the time we prioritize those who come here as a family to seek help because we encourage family involvement or partner involvement. So , if someone comes alone , we explore further to identify the reason she has come alone. That is when we identify the issues. We can say identification is accidental (HCW3) .
Qualified mental health professionals
Most participants acknowledged the importance of specialized mental health professionals who offer tailored and comprehensive assessments and psychological support that incorporate mothers’ specific psychosocial needs. For example,
S ome mothers needed counselling services and most of them would need psychosocial counselling and psychosocial counselling (which) would range from 1 week to up to 6 months and (this) needs qualified psychosocial counsellors (HCW 2).
Participants reported that at the time of the study, the hospital had only one mental health nurse working in the labor ward who was responsible for managing clients with severe mental illnesses. To address the issue of limited staff, some HCWs suggested a need for integration of mental health services into primary health care. It was suggested that this could be achieved by engaging non-mental health professionals to support mothers and implement early intervention. This would enable support to be provided to mothers immediately, which was especially important for young mothers, many of whom travel long distances, often on foot, to get to the clinic.
Another thing , is if we can have enough mental health personnel …for example , we only have 1 psychiatric nurse , the one who deals with all mental health issues… So , it will be ideal…if we have … a psychiatric nurse or anyone who looks into all those mental health conditions in the department like for example …. here at antenatal have one-person , general wards should have one and the other departments as well. That would help rather than just referring them to one person… It may happen that the person on that particular day is absent he is engaged with other issues so it means these people (adolescent with mental health issues) will not be assisted. And then telling them (adolescents) you should come another day will look like a burden to them. Looking at the distance they walk from home to here. I think that can be a problem. So…If we can have more mental health experts here (HCW 2) .
Health worker workforce
HCWs acknowledged the government of Malawi’s commitment to strengthen human resources for health including accelerating training and recruiting health professionals to support all positions required in the health sector. However, some HCWs also expressed concerns over the limited number of staff employed at the facility. Lack of staff was an issue, with the clinic treating around fifty mothers daily with only two nurses per shift, which tended to result in staff prioritizing physical health issues. Some HCWs and community volunteers suggested that community volunteers and community health workers can assist with screening mothers for mental health issues. Community volunteers concurred this would be feasible if they received appropriate training regarding screening procedures and mental health problems.
Given the workload at the clinic , little time is available to screen for mental disorders and hence they go unrecognized…they should be assisted (but) it is only the psychiatric nurse that decides the kind of medication. So , most of us will just look at the condition and we do not help much. We only focus on anemia , malaria , and pregnancy. Furthermore , community workers can assist with screening. (HCW 5).
Only if there was that opportunity for us (community volunteer) to learn how to teach about mental health and support mothers so that they could live without stress. We will be incredibly grateful because we will add more knowledge to what we already teach. ….and assist them properly (Community volunteerFGD1) .
Yes , we can use community workers or can find volunteers in the community who can identify people with mental issues and record their names and bring them to the hospital or provide mental health support (HCW 3).
Limited resources
Resource availability was cited as a facilitator for effectively delivering appropriate mental health services. Besides limited human resources, HCWs expressed concerns about the availability of other key resources to deliver the services. This theme has two subthemes: medication availability , lack of appropriate infrastructure. and competing priorities .
Medication availability
HCWs reported that all health services provided at the facility are free of charge. Hence, mothers do not pay for consultations and medication received at MRH. The faith-based organization St. John of God Hospitaller Services also partially supports mental health services with a free monthly mental health mobile clinic that provides medications for those with severe mental illnesses who attend the clinic on their clinic day. However, MRH provides perinatal and other outpatient services daily. Therefore, it was challenging for MRH to support mothers who required treatments on non-clinic days because MRH frequently experienced shortages of essential medications used to treat common mental disorders such as depression. HCWs attributed these shortages to limited government financing for medication and that mental health is not considered a priority by the authorities. Additionally, some HCWs also highlighted that medications safe for pregnant and lactating mothers were often not available, leaving some mothers untreated unless they could afford to pay for medication from the pharmacy.
Sometimes we have capacity , but we do not have resources. For example…. having safer antidepressants , we rarely have them …. we have the patients , but we are failing to put them on safe anti-depression medications… we could ask the family to buy , from pharmacies or private clinics… The situation is worse with mental health. No medication at all and we prioritize other medication (HCW 6) .
Lack of appropriate infrastructure
Some health workers expressed concern that the current hospital infrastructure does not allow for privacy, making some interventions difficult to implement. Rooms were difficult to access for private counselling sessions. The available open public spaces did not allow confidential discussions and did not have the capacity for partners to attend and accompany their spouses for labor, delivery, and clinic checkups. The need for privacy for mothers who had lost a baby was also emphasized by one participant who expressed concern that these mothers remained on the ward with other mothers and their babies.
Our hospital physical environment will not allow them (spouses/partners) to come…. postnatally …. they can’t be assisted well if they come with partners ……at least if the facility had rooms to provide privacy (HCW2).
We should have a separate room to deal with or to treat the mothers and give counselling because most of them would need psychosocial counselling and psychosocial counselling that would range from 1 week to up to 6 months and (this) needs privacy. (HCW3).
Particularly those that have lost their babies we need… a separate room for them because if we put them together with the mothers that have babies that brings in more mental disturbance…being traumatized (HCW6) .
Competing priorities
HCWs also expressed concerns over competing priorities with limited funding from the Malawi government and a lack of other non-government organizations and stakeholders supporting mental health services. Participants described how some health conditions receive special donor funding through specific projects. Some of these projects include funding of medication for communicable diseases such as malaria, sexually transmitted infections, and HIV/AIDS. However, there are currently no similar projects that fund mental health medications. This affects the availability of safe treatment options since government funding is insufficient to procure pregnancy-safe antidepressants. Further, during the COVID-19 pandemic, the situation worsened as funding and interventions shifted. For example, “We noticed that there is a lack of resources , particularly drugs because now the focus is on COVID-19 prevention supplies; this has affected the supply of other medications , including medication used during emergencies such as adrenaline” (HCW6”). Another health worker who was involved in providing mental health services stated:
We have patients who have chronic diseases such as epilepsy and mental illnesses , these have been affected more compared to patients that come for malaria or TB treatment Because malaria and TB have specific donors that supply medication but for epilepsy and mental health , we don’t have any medications (HCW3) .
Limited policy and guidelines implementation
Policy and guidelines were highlighted as facilitators to improved mental health care for women. Nurses and doctors acknowledged the availability of policies and guidelines regarding antenatal and postnatal care. However, the HCWs discussed the gap between these policies and their implementation. HCWs attributed gaps in implementation to issues such as fragmented care and inadequate financing for mental health services, insufficient workforce, unclear practical guidelines specific to maternal mental health care and a lack of staff orientation to new guidelines.
While the Ministry of Health had recently reviewed the antenatal guidelines and incorporated maternal mental health assessment, not all HCWs in this study were aware of these changes. Those who were aware reported that many staff were unfamiliar with recent guidelines. Some participants suggested the guidelines are not explicit, and HCWs require orientation to familiarize themselves with the changes. Furthermore, participants indicated that current antenatal policy does not clearly stipulate the mental health screening of postnatal mothers. HCWs suggested mental health screening should be mandatory.
Yes , the policies and guidelines might be there…so many people (nurses and clinicians) are not even aware of what is in the policies and to use them (policies)…Even the new anti-natal guidelines if you ask some nurses , they just know they are there but still practicing old ways where we only assess for physical problems like anemia , gestation age , and malaria (HCW1).
If you may ask me about motivational interviewing , and screening , I don’t know what it entails (HCW2).
I am personally not familiar with the changes; these were not disseminated to us. Orientation would help and for postnatal women we only assess for physical problems up to six weeks postnatal checkup. Probably screening should be mandatory (HCW 3) .
Cultural background and beliefs influence on help seeking
Adolescent mothers’ cultural backgrounds and beliefs impacted access to services. Broader community influence and traditional healer’s influence were sub-themes of this theme.
Broader community influence and beliefs
Traditional practitioners had different perceptions of how they described mental health problems. Mental health disorders were perceived to be the result of witchcraft or “someone just being silly” or “stupid”, with some participants in the traditional practitioners FGDs suggesting these issues do not warrant hospital treatment. The following quotes from herbalists and a spiritual healer support these sentiments:
Mental health conditions are because of stupidity mmm …Some people say it’s stupidity …but sometimes it’s indeed witchcraft (Herbalist FDG3).
You don’t think straight when you have mental issues. If such things happen , some say it is witchcraft , some say it is madness , and others say it’s Satanism. People talk a lot about these things (Spiritual healer FDG2).
……. aah! I think maybe we don’t know that this depression is a condition that can be treated if they can seek help… Only if we know that this is a disease can people go and seek medical help , but the problem is that people don’t know that this is a disease (Herbalist FDGs3).
Traditional practitioners discussed informal support provided within the community rather than the hospital. The discussion with community volunteers highlighted differing approaches. For example, a community volunteer shared an example of an adolescent mother who attempted suicide, refused to breastfeed and abandoned her baby. The mother was taken to the police as laws were broken, instead of being taken to the hospital for mental health support. Some community volunteers agreed with this, for example: When someone has dumped a baby because the mother is not thinking well … , hmm we take the mother to the police station so that the mother is punished” (Community volunteer FDG1). However, other participants focused on the safety of the child and the mother in this situation, for example: “It is because they fear for the life of that child. So , to protect their lives (the children) , they first go to the police station because if the child dies in their hands , they (the mothers) may be in trouble. We do not only want to get help for the baby but also save the life of the mother who dumped it. When you get to the police station , they tell you to go to the hospital” (Community volunteer FDG1).
Traditional healers influence
Traditional practitioners discussed providing mental health support within rural communities and the importance of traditional social support systems in the context of accessing mental health care. HCWs and traditional practitioners felt mothers seek help from spiritual healers, traditional healers or the health care system based on their perception of their health issue. Therefore, some community members consider traditional healing services the first point of contact for support.
Traditional practitioners reported that some adolescents with symptoms of mental health problems visit traditional practitioners for ‘ breaking of spells’ , a spell being cast by ancestor’s spirits upon the person for wrongdoing with mental health problems as a form of punishment. One traditional healer commented: “Some of the mental health disorders come when the adolescent’s parents or ancestors did not follow some rituals , and therefore , they are spiritually tied like a chain…. and this is like a covenant…… and therefore it runs in the families , and these can only be healed by breaking the chain…. another one echoed this sentiment: “They are spells from their ancestors , they can only be healed through exhortation” (Traditional healer FGD3) . A spiritual healer brought a different dimension to dealing with mental issues. For example, one spiritual healer recounted an incident whereby a girl visited the spiritual healer with issues, and the healer felt the girl’s mental health issues were because she was “thinking too much”: “I had a certain girl at home who was 7 months pregnant. She was always worried when she came to me , she never opened up. I do not have a clinic , but I practice spiritual healing. She came to me and said you should test me…so I asked her what I should check on. She said just check me. When I consulted the spirits , they told me that the girl has no problems in her life , but she thinks a lot because of her wrongdoing so she should stop that. I told her that when she stopped thinking a lot , her health would improve (Spiritual healer FGD2). Similarly, another spiritual healer discussed encouraging mothers to talk, pray and make peace with others to alleviate mental health problems:
When someone with worries comes to me , we encourage each other by talking with them through prayers. Then we advise the person on how to behave where she is staying with her neighbours…If some people were not talking to her , she should be the first to open up by starting with greeting them. When they do that , they come back here to give a testimony…God has helped in resolving the disputes! And most mothers say that …. I thank God and praise him for what He has done because I never thought I would ever be happy again , but your prayers and my prayers have worked. God has answered the prayers (Spiritual healer FGD2) .
In addition, traditional practitioners across all three groups perceived that sometimes, HCWs’ attitude encourages mothers to opt to seek help from traditional healers and other community-based informal providers for their mental health problems rather than HCWs. Traditional practitioners reported that the reception people receive when they visit the hospital is not always positive. For example, in FGD3 with traditional healers, one traditional healer, a traditional birth attendant, stated “ Health workers are the biggest problem , so let us be open here. Instead of welcoming and assisting us based on our feelings , you treat us badly… (Traditional birth attendant FGD3). Another Herbalist stated sometimes you (health workers) take too long to assist someone…instead of assessing someone to know how they are , you are busy chatting or sliding your smartphones (Herbalist FGD3). Similarly, a spiritual healer in FGD2 stated when adolescents come to us (spiritual healers) , we pray for them , sit down with them , and hold their hands. However , in hospitals , the care is left to cleaners , who sometimes send them back even without seeing a professional health worke r (S piritual healer FGD2) . Given these experiences some traditional practitioners discussed the need to provide better and more compassionate care than hospitals. For example:
Even though you (health workers) do not allow women to deliver at traditional caregivers… more women around this hospital prefer to go there because they are treated well. The treatment we get from the traditional caregivers and here at the hospital is very different because of the behaviour of the people who work at the hospitals (Traditional birth attendant FGD2 ).
If you put the nurses and the traditional caregivers here and compare them , you will see that we manage to help people deliver babies properly in the villages. We treat people very well but at the hospital they are very cruel, they shout at pregnant women (Traditional birth attendant FGD2 ).
Notably, all participants from the FGDs and in-depth interviews discussed the need to collaborate with each other. Traditional practitioners felt that traditional healers and birth attendants should refer clients to the hospital. In addition, all traditional practitioners, including community volunteers, wanted more mental health training to enhance their confidence to identify and refer clients with potential mental health problems to the hospital. Participants discussed that while mental health support can be provided by different groups, such as the church, community volunteers, traditional birth attendants, and other people within the community, it was important that mothers experiencing mental health problems were referred to the hospital. HCWs emphasized that proper sensitization and awareness of traditional practitioners and the community around mental health issues is very important due to traditional practitioners’ limited knowledge and skills about maternal mental health. There was a general agreement that task sharing with collaboration is more important than working in isolation. Participants felt utilizing current community structures (community health workers, community health volunteers, and village health committees) would assist in extending support to more mothers. For example:
The traditional healers and government health workers should work together so that we should encourage the pregnant girls with such conditions (mental health problems) to go to the hospital. So that when they give birth to their baby they can go back to school , and this will ensure a better future for those young people and if we see that the girl needs counselling , we should take them to the hospital. We should work together because we are all helping people (Herbalist FGD3) .
I hope the best lesson is that we should work together , we are all helping people including girls. Sometimes we are ignorant of some things , do not neglect us, give us trainings so that we refer clients to each other when we meet somethings that we cannot manage. (Traditional Birth Attendant FGD2)
This is the first study to explore access to maternal mental health of adolescent mothers in Malawi. Access to mental health care services by adolescent mothers remains a challenge in most LMICs [ 55 , 56 ], and the reasons are multifaceted. In this Malawian study, HCW’s competence in mental health assessment, lack of a culturally appropriate screening tool, limited resources, and cultural and community influences were the perceived factors that impacted access to maternal mental health. Studies conducted in Uganda, Liberia and Nepal around barriers to accessing mental health support for people with mental health problems reported similar findings [ 57 , 58 ]. In South Africa, the reasons that contributed to poor access to maternal mental health were attributed to systemic health issues such as structural stigma, for example, not implementing appropriate mental health policies, cultural background of mothers, particularly beliefs about the causes of mental health disorders, and health workers competence [ 11 , 59 ]. Comprehensive access to mental health care requires a multifaceted and holistic approach, highlighting the need to improve mental health literacy and skills among HCWs and traditional practitioners and to address systemic barriers.
While HCWs in this study acknowledged the importance of screening as an essential intervention for early identification and treatment, screening of mothers for mental health problems was challenging. This finding is similar to studies conducted in Kenya and Ghana where health workers also reported challenges in providing screening services due to a lack of training around the conduct of maternal mental health assessments and the lack of a formal process to screen women for postnatal depression [ 26 , 56 , 60 ]. In Malawi, limited competencies among HCWs may be attributed to inadequacies within the current health workers’ pre-service training curriculum. These findings call for a review of the current Malawian nursing and medical curriculum to incorporate modules focusing on screening for common mental disorders in perinatal women. In addition, in-service training for health workers around the implementation of maternal mental health screening tools is essential to improve health workers’ confidence in the provision of comprehensive screening and management.
The findings of this study highlight that insufficient numbers of mental health professionals resulted in fewer opportunities for ongoing support, and long waiting times for mothers to access mental health support. Some studies suggest task shifting to be a strategy to increase access [ 26 ]. This involves psychological therapies being provided by non- trained health workers [ 61 ] or where tasks are shifted from professionals to community volunteers with fewer qualifications [ 62 , 63 ], thereby increasing reach [ 60 , 64 ]. For example, a literature review focusing on the implementation of task sharing in LMICs, where there are limited health workers, has found improved access to mental health support [ 65 ]. In Malawi, community health workers, informal health care providers, and community health volunteers are embedded within the community setting. These existing personnel and the current organizational structure may provide opportunities for task sharing [ 60 ]. For example, in Malawi, community links with the primary care facility via a team of health surveillance assistants (HSAs), community health workers (CHWs) and traditional healers is possible. HSAs are community-level cadres who receive six weeks of initial training and supervise community volunteers. HSAs and community volunteers provide health promotion and preventive health care through door-to-door visitations and outreach clinics and are supervised by community nurses and public health officers. Each HSA is responsible for a population of 1500, and each village has a volunteer [ 66 ]. In this study, HCWs and traditional practitioners suggested a task-sharing approach to provide effective assistance. However, they felt that orientation and training would be necessary considering the complexity of maternal mental health problems and some of the different belief systems and ways of working between HCWs and traditional practitioners. It was evident in this study that traditional practitioners play an important role in the health care of young mothers in Malawi, with many providing examples of support which could be enhanced by training. In addition, policy makers should consider deploying mental health workers in maternal health departments to provide support to adolescent mothers.
Limited resources in terms of infrastructure and competing priorities were also discussed as barriers to the availability of mental health services. These factors affect the type of support available to adolescent mothers. For example, adequate and appropriate infrastructure provides privacy for therapeutic communication and counselling [ 55 ]. Lack of infrastructure creates difficulties for both service providers and the consumers of mental health services to render and access appropriate services [ 55 ]. Similarly, participants in this study felt that improving the current infrastructure may create a conducive environment that may support adolescent mothers.
Participants in this study highlighted the importance of mental health policy. They felt policies and guidelines on maternal mental health screening in Malawi were not explicit and not well implemented. A lack of policy implementation may contribute to inequality in resource allocation, leading to the diversion of attention and resources, which may result in poor funding of services tailored for maternal mental health. Some authors attribute this to structural stigma within the health system, which affects funding and resource allocation [ 24 , 65 , 67 , 68 ]. Therefore, research on effective and efficient mental health interventions would inform policymakers on evidence-based, cost-effective interventions that are appropriate for perinatal women. For example, adopting task sharing using existing community structures and traditional health workers, including community volunteers, could be trialed. Furthermore, policy reviews and enforcement around the implementation of policy may provide support for funding and hence result in improvements in maternal mental health service delivery [ 69 ]. The inclusion of screening guidelines in policies would emphasize the need for mental health screening into the postnatal period and facilitate financing for its implementation.
There is ongoing debate on the integration of spirituality or religiosity into the management of people experiencing mental health problems. However, evidence from programs in HIC has found that integrating religious elements into therapy is beneficial for some patients [ 70 ]. In the Sub-Saharan African context, [ 56 , 71 ] and consistent with the findings of this study, traditional practitioners highlighted the benefits of spirituality. Participants in this study did, however, discuss differing beliefs that impacted care. HCWs discussed their biopsychosocial explanation of mental disorders, while some traditional practitioners discussed their belief that bad spirits or being cursed causes mental disorders. These differing beliefs may cause mistrust between HCWs and traditional practitioners. In our study, spiritual healing was reported to assist adolescent mothers in considering life as sacred and meaningful, and as such, was an essential part of the recovery process, with spiritual healers providing alternative coping methods that are essential for healing. Our study also found adolescent mothers who were experiencing mental health difficulties were more likely to be prayerful and hence receptive to intervention from traditional practitioners [ 6 ]. These findings highlight the importance of collaborating and supporting religious leaders and other traditional practitioners.
Strengths and limitations
This study was conducted in a rural setting in Malawi in one hospital catchment area. While findings are unique to this setting, they may be of interest to other regions of Malawi and other SSA countries. The perceptions of HCWs and traditional practitioners provide a unique contribution to the understanding of access and availability of mental health support for adolescent mothers. Despite being conducted during the COVID-19 pandemic, 30 traditional practitioners were recruited. All six HCWs at the MCH at MRH consented to participate in the study.
Conclusion and recommendations
Access to mental health care support for adolescent mothers in Malawi appears to be impacted by inadequate staff development, limited resources, limited policy and guidelines implementation, and cultural background and beliefs influences on help-seeking. Enhancing mental health literacy among HCWs and traditional practitioners is important to improve their understanding of mental health issues. Training of health workers should include mandatory screening for common mental disorders for pregnant and postnatal adolescents using standard, locally validated screening tools to ensure that mental health problems are detected early. Furthermore, training in empathetic communication skills to improve communication would be essential.
Health facilities should co-develop and implement coordinated interventions with community stakeholders to strengthen community engagement initiatives between HCWs and traditional practitioners with the aim of improving support for adolescent mothers.
Advocacy is required to encourage the Government of Malawi to increase funding for mental health services. Funding is needed to access medications, enhance infrastructure and support policy implementation. Critically staffing increase, especially for mental health nurses, is essential.
Lastly, future research should evaluate the efficacy and effectiveness of interventions that promote help-seeking, enhance prevention, early detection, and timely treatment, utilizing HCWs and traditional practitioners as referral points. For example, research on providing interventions through task sharing would be beneficial.
Availability of data and materials
Data are hosted by the Curtin University survey office through the Human Research Ethics Committee. Researchers who meet the criteria for access to confidential data can request it through the Chairperson Ethics Committee, and the data will be made available.
Umuziga MP, Adejumo O, Hynie M. A cross-sectional study of the prevalence and factors associated with symptoms of perinatal depression and anxiety in Rwanda. BMC Pregnancy Childbirth. 2020;20(1):68.
Article PubMed PubMed Central Google Scholar
Fisher J, Cabral de Mello M, Patel V, Rahman A, Tran T, Holton S, et al. Prevalence and determinants of common perinatal mental disorders in women in low- and lower-middle-income countries: a systematic review. Bull World Health Organ. 2012;90(2):g139–49.
Article Google Scholar
Hartley M, Tomlinson M, Greco E, Comulada WS, Stewart J, Le Roux I, et al. Depressed mood in pregnancy: prevalence and correlates in two Cape Town peri-urban settlements. Reprod Health. 2011;8(1):9.
Chorwe-Sungani G, Chipps J. Performance of the 3-item screener, the Edinburgh Postnatal Depression Scale, the Hopkins symptoms Checklist-15 and the self-reporting questionnaire and pregnancy risk questionnaire, in screening of depression in antenatal clinics in the Blantyre district of Malawi. Malawi Med J. 2018;30(3):184–90.
Stewart RC, Bunn J, Vokhiwa M, Umar E, Kauye F, Fitzgerald M, et al. Common mental disorder and associated factors amongst women with young infants in rural Malawi. Soc Psychiatry Psychiatr Epidemiol. 2010;45(5):551–9.
Article PubMed Google Scholar
Tembo C, Portsmouth L, Burns S. Postnatal depression and its social-cultural influences among adolescent mothers: a cross sectional study. PLOS Glob Public Health. 2023;3(6):e0002025.
Steventon Roberts KJ, Smith C, Cluver L, Toska E, Jochim J, Wittesaele C, et al. Adolescent mothers and their children affected by HIV-An exploration of maternal mental health, and child cognitive development. PLoS One. 2022;17(10):e0275805.
Article PubMed PubMed Central CAS Google Scholar
Eccles J, Templeton J, Barber B, Stone M. Adolescence and emerging adulthood: the critical passage ways to adulthood. 2003.
Google Scholar
Ahorlu CK, Pfeiffer C, Obrist B. Socio-cultural and economic factors influencing adolescents’ resilience against the threat of teenage pregnancy: a cross-sectional survey in Accra, Ghana. Reprod Health. 2015;12:117.
Swift ER, Pierce M, Hope H, Osam CS, Abel KM. Young women are the most vulnerable to postpartum mental illness: a retrospective cohort study in UK primary care. J Affect Disord. 2020;277:218–24.
Aguirre Velasco A, Cruz ISS, Billings J, Jimenez M, Rowe S. What are the barriers, facilitators and interventions targeting help-seeking behaviours for common mental health problems in adolescents? A systematic review. BMC Psychiatry. 2020;20(1):293.
Baron EC, Hanlon C, Mall S, Honikman S, Breuer E, Kathree T, et al. Maternal mental health in primary care in five low- and middle-income countries: a situational analysis. BMC Health Serv Res. 2016;16(1):53.
Stewart RC, Umar E, Kauye F, Bunn J, Vokhiwa M, Fitzgerald M, et al. Maternal common mental disorder and infant growth–a cross-sectional study from Malawi. Matern Child Nutr. 2008;4(3):209–19.
Carbone NB, Njala J, Jackson DJ, Eliya MT, Chilangwa C, Tseka J, et al. I would love if there was a young woman to encourage us, to ease our anxiety which we would have if we were alone: adapting the Mothers2Mothers Mentor Mother Model for adolescent mothers living with HIV in Malawi. PLoS One. 2019;14(6):e0217693.
Levesque J-F, Harris MF, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013;12(1):18.
Mutahi J, Larsen A, Cuijpers P, Peterson SS, Unutzer J, McKay M et al. Mental health problems and service gaps experienced by pregnant adolescents and young women in Sub-saharan Africa: a systematic review. eClinicalMedicine. 2022;44:101289.
Heyningen Tv, Myer L, Onah M, Tomlinson M, Field S, Honikman S. Antenatal depression and adversity in urban South Africa. J Affect Disord. 2016;203:121–9.
Udedi M. Improving access to mental health services in Malawi. 2017.
The Governement of Malawi. National mental health, policy April 2020. In: Health TMo. 2nd ed. Lilongwe: Governement print; 2020.
The Ministry of Health. Mental health policy. 2020.
Field T. Postnatal anxiety prevalence, predictors and effects on development: a narrative review. Infant Behav Dev. 2018;51:24–32.
Hom MA, Stanley IH, Joiner TE Jr. Evaluating factors and interventions that influence help-seeking and mental health service utilization among suicidal individuals: a review of the literature. Clin Psychol Rev. 2015;40:28–39.
Gureje O, Kola L, Oladeji BD, Abdulmalik J, Ayinde O, Zelkowitz P, et al. Responding to the challenge of adolescent Perinatal Depression (RAPiD): protocol for a cluster randomized hybrid trial of psychosocial intervention in primary maternal care. Trials. 2020;21(1):1–11.
Field S, Abrahams Z, Honikman S. Adolescent mothers: a qualitative study on barriers and facilitators to mental health in a low-resource setting in Cape Town, South Africa. Afr J Prim Health Care Fam Med. 2020;12:1–9.
Tembo C, Burns S, Portsmouth L. Maternal mental health of adolescent mothers: a cross-sectional mixed-method study protocol to determine cultural and social factors and mental health needs in Lilongwe, Malawi. BMJ Open. 2022;12(5):e056765.
McCauley M, Brown A, Ofosu B, van den Broek N. I just wish it becomes part of routine care: healthcare providers’ knowledge, attitudes and perceptions of screening for maternal mental health during and after pregnancy: a qualitative study. BMC Psychiatry. 2019;19(1):279.
Ng’oma M, Meltzer-Brody S, Chirwa E, Stewart RC. Passing through difficult times: perceptions of perinatal depression and treatment needs in Malawi-A qualitative study to inform the development of a culturally sensitive intervention. PLoS One. 2019;14(6):e0217102.
Alhasel HMB, Abdelgadir HS, Alshehri AAA. Effectiveness of psychological intervention in management of postpartum depression. Egypt J Hosp Med. 2018;70(12):2157–61.
El-Den S, O’Reilly CL, Chen TF. A systematic review on the acceptability of perinatal depression screening. J Affect Disord. 2015;188:284–303.
Nunes AP, Phipps MG. Postpartum depression in adolescent and adult mothers: comparing prenatal risk factors and predictive models. Matern Child Health J. 2013;17:1071–9.
Zamawe C, King C, Jennings HM, Fottrell E. Associations between the use of herbal medicines and adverse pregnancy outcomes in rural Malawi: a secondary analysis of randomised controlled trial data. BMC Complement Altern Med. 2018;18(1):1–8.
Barnes LAJ, Barclay L, McCaffery K, Aslani P. Complementary medicine products used in pregnancy and lactation and an examination of the information sources accessed pertaining to maternal health literacy: a systematic review of qualitative studies. BMC Complement Altern Med. 2018;18(1):229.
Crabb J, et al. Attitudes towards mental illness in Malawi: a cross-sectional survey. BMC Public Health. 2012;1(12):541.
Mureyi DD, Monera TG, Maponga CC. Prevalence and patterns of prenatal use of traditional medicine among women at selected harare clinics: a cross-sectional study. BMC Complement Altern Med. 2012;12:1–7.
Nergard CS, Ho TPT, Diallo D, Ballo N, Paulsen BS, Nordeng H. Attitudes and use of medicinal plants during pregnancy among women at health care centers in three regions of Mali, West-Africa. J Ethnobiol Ethnomed. 2015;11:1–11.
WHO Adolescent pregnancy. Fact sheet World health organization. 2018. Updated January 2018.
Gilmore B, McAuliffe E. Effectiveness of community health workers delivering preventive interventions for maternal and child health in low- and middle-income countries: a systematic review. BMC Public Health. 2013;13:847.
ICF Na. Malawi demographic and health survey 2015–16. Zomba and Rockville. 2017.
The Malawi Government. List of Hospitals In: Health, editor. Government print. 2005.
Rutledge PB, Hogg JLC. In-Depth Interviews. The International Encyclopedia of Media Psychology. 2020. pp. 1–7.
Zaharia RM, Alin S. Qualitative research methods: a comparison between focus group and indept interviews. 2008.
O.Nyumba T, Wilson K, Derrick CJ, Mukherjee N. The use of focus group discussion methodology: insights from two decades of application in conservation. Methods Ecol Evol. 2018;9(1):20–32.
Johnstone M-L. Depth interviews and focus groups. In: Kubacki K, Rundle-Thiele S, editors. Formative Research in Social Marketing: innovative methods to Gain Consumer insights. Singapore: Springer Singapore; 2017. pp. 67–87.
Chapter Google Scholar
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57.
Land L, Harvey M. Research methods for nurses and midwives: theory and practice. Res Methods Nurs Midwives. 2021;2:1-100.
Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82.
Creswell JW, Sinley RC. Developing a culturally-specific mixed methods approach to global research. Kölner Zeitschrift für Soziologie Und Sozialpsychologie. 2017;69(Supplement 2):87–105.
Kalu FA, Bwalya JC. What makes qualitative research good research? An exploratory analysis of critical elements. Int J Soc Sci Res. 2017;5(2):43–56.
Guo JX. Measuring information system project success through a software-assisted qualitative content analysis. Inform Technol Libr. 2019;38(1):53–70.
Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Res Psychol. 2006;3(2):77–101.
Braun V, Clarke V. Contextualism. Thematic analysis a practical guide. London: Sage; 2022.
Maguire M, Delahunt B. Doing a thematic analysis: a practical, step-by-step guide for learning and teaching scholars. All Irel J High Educ. 2017;9(3).
Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–40.
Article PubMed CAS Google Scholar
Korstjens I, Moser A, Series. Practical guidance to qualitative research. Part 4: trustworthiness and publishing. Eur J Gen Pract. 2017;24(1):120–4.
Strumpher J, Van Rooyen RM, Topper K, Andersson LMC, Schierenback I. Barriers to accessing mental health care in the Eastern Cape province of South Africa. Afr J Nurs Midwifery. 2014;16(1):45–59.
Goyal D, Rabemananjara KM, Lara-Cinisomo S, Le H-N. Healthcare worker’s understanding of perinatal depression and maternal mental health service needs in rural Kenya. Mental Health Prev. 2023;29:200260.
Moskos MA, Olson L, Halbern SR, Gray D. Utah youth suicide study: barriers to mental health treatment for adolescents. Suicide Life Threat Behav. 2007;37(2):179–86.
Kisa R, Baingana F, Kajungu R, Mangen PO, Angdembe M, Gwaikolo W, et al. Pathways and access to mental health care services by persons living with severe mental disorders and epilepsy in Uganda, Liberia and Nepal: a qualitative study. BMC Psychiatry. 2016;16(1):305.
Kathree T, Selohilwe OM, Bhana A, Petersen I. Perceptions of postnatal depression and health care needs in a South African sample: the mental in maternal health care. BMC Womens Health. 2014;14(1):140.
Musyimi CW, Mutiso VN, Ndetei DM, Unanue I, Desai D, Patel SG, et al. Mental health treatment in Kenya: task-sharing challenges and opportunities among informal health providers. Int J Ment Health Syst. 2017;11:45.
Clarke K, King M, Prost A. Psychosocial interventions for Perinatal Common Mental disorders delivered by Providers who are not Mental Health specialists in low- and Middle-Income countries: a systematic review and Meta-analysis. PLoS Med. 2013;10(10):e1001541.
Atif N, Lovell K, Husain N, Sikander S, Patel V, Rahman A. Barefoot therapists: barriers and facilitators to delivering maternal mental health care through peer volunteers in Pakistan: a qualitative study. Int J Ment Health Syst. 2016;10:24.
Petersen I, Lund C, Bhana A, Flisher AJ, Mental H, Poverty Research Programme C. A task shifting approach to primary mental health care for adults in South Africa: human resource requirements and costs for rural settings. Health Policy Plan. 2012;27(1):42–51.
Schaffer M, Goodhue A, Stennes K, Lanigan C. Evaluation of a Public Health Nurse Visiting Program for Pregnant and parenting teens. Public Health Nurs (Boston Mass). 2012;29:218–31.
Zhu Y, Ma J, Wang Q, Xu Y, Xu G, Du S. Factors affecting the implementation of task-sharing interventions for perinatal depression in low- and middle-income countries: a systematic review and qualitative metasynthesis. J Affect Disord. 2022;300:400–9.
Makwero M. Delivery of primary health care in Malawi. Afr J Prim Health Care Fam Med. 2018;10(1):e1–3.
Shahabuddin A, Nöstlinger C, Delvaux T, Sarker M, Delamou A, Bardají A, et al. Exploring maternal Health Care-seeking behavior of married adolescent girls in Bangladesh: a social-ecological approach. PLoS One. 2017;12(1):e0169109.
Tesfaye Y, Agenagnew L, Anand S, Tucho GT, Birhanu Z, Ahmed G, et al. Knowledge of the community regarding mental health problems: a cross-sectional study. BMC Psychol. 2021;9(1):106.
Chisholm D, Docrat S, Abdulmalik J, Alem A, Gureje O, Gurung D, et al. Mental health financing challenges, opportunities and strategies in low-and middle-income countries: findings from the Emerald project. BJPsych Open. 2019;5(5):e68.
Hefti R. Integrating religion and spirituality into mental health care, psychiatry and psychotherapy. Religions. 2011;2(4):611–27.
Adeponle A, Groleau D, Kola L, Kirmayer LJ, Gureje O. Perinatal depression in Nigeria: perspectives of women, family caregivers and health care providers. Int J Mental Health Syst. 2017;11(1):27.
Download references
Acknowledgements
The authors acknowledge the support of the head of the School of Population Health, Curtin University for scholarship support, the Lilongwe District Health Officer, and his team for accepting us to conduct the study and the Clinic in charge for the coordination. I would also like to acknowledge the support of Margret Zgambo, Precious Kachale, Dr Saulos Gondwe, and Charles Ndawala for your support during data collection.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The author secured a Research Training Stipend Scholarship for doctoral studies. From Curtin University.
Author information
Authors and affiliations.
Saint John of God Hospitaller services, Mzuzu, Malawi
Chimwemwe Tembo
School of Population Health, Faculty of Health Sciences, Curtin University, Perth, Australia
Linda Portsmouth & Sharyn Burns
You can also search for this author in PubMed Google Scholar
Contributions
CT came up with the idea for the study, while SB and LP, who served as supervisors, gave it a critical assessment, and enlarged it. CT, SB, and LP conceptualized the study. Data curation was done by CT, L P, and SB. Supervision and formal analysis of data were done by all authors. All authors reviewed the manuscript.
Authors’ information
The corresponding author (CT) is a mental health nurse with an interest in the mental health promotion of women and a Malawi representative for the African Alliance for Maternal Mental Health. She works with St John of God Malawi as a community mental health coordinator and is a PhD student at Curtin University in Australia and is supervised by Professor Sharyn Burns (PhD, MPH, BEd) and Dr Linda Portsmouth (PhD, MHlthComm, BAppSc).
Corresponding author
Correspondence to Chimwemwe Tembo .
Ethics declarations
Ethics approval and consent to participate.
Ethical approval was received from the Curtin University Human Research Ethics Committee (HRE2021-0223) and the Malawi National Committee on Research Ethics in the Social Sciences and Humanities (P.05/21/575).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., supplementary material 2., supplementary material 3., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Tembo, C., Portsmouth, L. & Burns, S. Identification of mothers with mental health problems is accidental: perceptions of health care providers on availability, access, and support for maternal mental health care for adolescent mothers in Malawi. BMC Health Serv Res 24 , 983 (2024). https://doi.org/10.1186/s12913-024-11469-z
Download citation
Received : 14 May 2024
Accepted : 20 August 2024
Published : 26 August 2024
DOI : https://doi.org/10.1186/s12913-024-11469-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Mental health services
- Access to mental health
- Adolescent mothers
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]
Qualitative Risk Assessment Methods
- First Online: 25 July 2023
Cite this chapter

- Eric Liberda 3 &
- Timothy Sly 3
229 Accesses
Although the primary “risk assessment” focus of this book addresses quantitative methods, several qualitative methods of risk analysis are widely used for evaluation and decision-making across all industrial, institutional, educational, and commercial organizations.
Qualitative analysis methods describe risks in relative terms, without introducing complex calculations or requiring computing of probabilities. Numbers are sometimes used but only to rank a risk as being relatively higher or lower than another risk, or establishing a priority for remediation or resolution.
This chapter offers an introduction with examples and applications for the following qualitative processes.
Preliminary Risk Analysis (PRA)
Failure Mode Effects Analysis (FMEA)
Fault tree analysis (FTA)
Management Oversight and Fault Tree (MORT)
Hazard and Operability (HAZOP)
Hazard Analysis, Critical Control Point (HACCP) is also a qualitative risk analysis method that has been included in Chap. 5 because of its original and continued association with food safety.
This is not an exhaustive list by any means, but it gives an idea of the types and applications of these useful and common methods of analyzing risks in almost any setting. Support for learning and developing qualitative techniques is well served by instructional facilities, traditional and online training programs, expertise, extension programs, and resources from both private and public sectors. Further readings and references are supplied at the end of the chapter.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
Subscribe and save.
- Get 10 units per month
- Download Article/Chapter or eBook
- 1 Unit = 1 Article or 1 Chapter
- Cancel anytime
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
ICMA. International Crisis Management Association. Management oversight and risk tree (MORT). http://icma.org.uk/06-9_mort.html . Accessed Nov 2022.
OSHA. FactSheet: the importance of root cause analysis during incident investigation. 2016. https://www.osha.gov/sites/default/files/publications/OSHA3895.pdf . Accessed Dec 2022.
SAE. Fault/failure analysis procedure: design analysis procedure for failure modes, effects and criticality analysis (FMECA). Society for Automotive Engineers ARP926C. Feb 2018.
Google Scholar
US DHHS. Root cause analysis. US Department of Health & Human Services. 7 Sept 2019. https://psnet.ahrq.gov/primer/root-cause-analysis . Accessed Dec 2022.
Download references
Author information
Authors and affiliations.
School of Occupational & Public Health and School of Graduate Studies, Toronto Metropolitan University, Toronto, ON, Canada
Eric Liberda & Timothy Sly
You can also search for this author in PubMed Google Scholar
Rights and permissions
Reprints and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter
Liberda, E., Sly, T. (2023). Qualitative Risk Assessment Methods. In: Assessment and Communication of Risk. Springer, Cham. https://doi.org/10.1007/978-3-031-28905-7_4
Download citation
DOI : https://doi.org/10.1007/978-3-031-28905-7_4
Published : 25 July 2023
Publisher Name : Springer, Cham
Print ISBN : 978-3-031-28904-0
Online ISBN : 978-3-031-28905-7
eBook Packages : Medicine Medicine (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
- Search Search Please fill out this field.
What Is Risk Assessment?
Understanding risk assessment, risk assessments for investments, risk assessments for lending, risk assessments for business.
- Fundamental Analysis
Risk Assessment Definition, Methods, Qualitative Vs. Quantitative
:max_bytes(150000):strip_icc():format(webp)/wk_headshot_aug_2018_02__william_kenton-5bfc261446e0fb005118afc9.jpg "risk assessment qualitative research")
Risk assessment is a general term used across many industries to determine the likelihood of loss on an asset, loan, or investment. Assessing risk is essential for determining how worthwhile a specific investment is and the best process(es) to mitigate risk. It presents the upside reward compared to the risk profile . Risk assessment is important in order to determine the rate of return an investor would need to earn to deem an investment worth the potential risk.
Key Takeaways
- Risk assessment is the process of analyzing potential events that may result in the loss of an asset, loan, or investment.
- Companies, governments, and investors conduct risk assessments before embarking on a new project, business, or investment.
- Quantitative risk analysis uses mathematical models and simulations to assign numerical values to risk.
- Qualitative risk analysis relies on a person's subjective judgment to build a theoretical model of risk for a given scenario.
- While a stock's past volatility does not guarantee future returns, in general, an investment with high volatility indicates a riskier investment.
Risk assessment enables corporations, governments, and investors to assess the probability that an adverse event might negatively impact a business, economy, project, or investment. Risk analysis provides different approaches investors can use to assess the risk of a potential investment opportunity. Two types of risk analysis an investor can apply when evaluating an investment are quantitative analysis and qualitative analysis.
Quantitative Analysis
A quantitative analysis of risk focuses on building risk models and simulations that enable the user to assign numerical values to risk. An example of quantitative risk analysis would be a Monte Carlo simulation . This method—which can be used in a variety of fields such as finance, engineering, and science—runs a number of variables through a mathematical model to discover the different possible outcomes.
Qualitative Analysis
A qualitative analysis of risk is an analytical method that does not rely on numerical or mathematical analysis. Instead, it uses a person's subjective judgment and experience to build a theoretical model of risk for a given scenario. A qualitative analysis of a company might include an assessment of the company's management, the relationship it has with its vendors, and the public's perception of the company.
Investors frequently use qualitative and quantitative analysis in conjunction with one another to provide a clearer picture of a company's potential as an investment.
Other Risk Assessment Methods
Another example of a formal risk assessment technique includes conditional value at risk (CVaR) , which portfolio managers use to reduce the likelihood of incurring large losses. Mortgage lenders use loan-to-value ratios to evaluate the risk of lending funds. Lenders also use credit analysis to determine the creditworthiness of the borrower.
Both institutional and individual investments have expected amounts of risk. This is especially true of non-guaranteed investments, such as stocks, bonds, mutual funds , and exchange-traded funds (ETFs) .
Standard deviation is a measure applied to the annual rate of return of an investment to measure the investment's volatility . In most cases, an investment with high volatility indicates a riskier investment. When deciding between several stocks, investors will often compare the standard deviation of each stock before making an investment decision.
However, it's important to note that a stock's past volatility (or lack thereof) does not predict future returns. Investments that previously experienced low volatility can experience sharp fluctuations, particularly during rapidly changing market conditions.
Lenders for personal loans, lines of credit , and mortgages also conduct risk assessments, known as credit checks. For example, it is common that lenders will not approve borrowers who have credit scores below 600 because lower scores are indicative of poor credit practices. A lender's credit analysis of a borrower may consider other factors, such as available assets, collateral , income, or cash on hand.
Business risks are vast and vary across industries. Such risks include new competitors entering the market; employee theft; data breaches; product recalls; operational, strategic and financial risks; and natural disaster risks.
Every business should have a risk management process in place to assess its current risk levels and enforce procedures to mitigate the worst possible risks. An effective risk management strategy seeks to find a balance between protecting the company from potential risks without hindering growth. Investors prefer to invest in companies that have a history of good risk management.
:max_bytes(150000):strip_icc():format(webp)/usa---natural-disasters---kansas-tornado-aftermath-524640304-b28a5ddbea3a43c98aa1126fcda12072.jpg "risk assessment qualitative research")
- Terms of Service
- Editorial Policy
- Privacy Policy
- Your Privacy Choices

Home / Resources / News and Trends / ISACA Now Blog / 2021 / Qualitative vs Quantitative Risk Assessment
Qualitative vs. quantitative risk assessment.

With the ongoing impact of the COVID-19 pandemic in today’s business ecosystem, the value of decision making by using risk-oriented thinking has emerged more clearly and precisely. There is not a field of business that does not feel the contribution of risk assessment results, from information security to business continuity and resilience.
One of the most difficult decisions for a risk practitioner or risk manager is determing the most appropriate assessment method to use in the risk analysis process. Many different risk analysis methods have been used effectively and efficiently over the years. However, it can be challenging to make the final decision depending on the character of the asset/process subject to risk and the type and size of the risk-related data available.
In general, it is neccessary to first understand how to use risk-based thinking. Then, it becomes easier to decide which risk analysis can make the highest contribution to risk assessment, depending on an organization’s expertise in business processes, the technological infrastructure, the tools used and the quality and reliability of the data available.
First, the relationships between assets, processes, threats, vulnerabilities and other factors are analyzed in the risk assessment approach. There are many methods available, but quantitative and qualitative analysis are the most widely known and used classifications.
Qualitative risk analysis can be generally performed on all business risk. The qualitative approach is used to quickly identify risk areas related to normal business functions. Although the biased attitudes of staff or the lack of work experience can sometimes make the process difficult, qualitative risk analysis generally strengthens an effective risk assessment approach.
If there is an environment where decisions must be made based on data, it would be the most logical decision to use quantitative risk analysis methods. Quantitative risk analysis provides more objective information and accurate data than qualitative analysis because quantitative risk assessment is based on realistic and measurable data used to calculate the impact values that the risk will create with the probability of occurrence. The most common problem in quantitative assessment is that there is not enough data to be analyzed. There also can be challenges in revealing the subject of the evaluation with numerical values or the number of relevant variables is too high. This makes risk analysis technically difficult.
When determining whether to use a quantitative or a qualitative approach, you will find positives and negatives to both options. Qualitative risk assessment is quick to implement due to the lack of statistical/numerical dependence and measurements, and can be performed easily. It is also beneficial if employees are experienced in asset/processes; however, they may also bring biases in determining probability and impact. Qualitative risk analysis is quick but subjective. On the other hand, quantitative risk analysis is objective and has more detail, contingency reserves and go/no go decisions, but it takes more time and is more complex. Quantitative data are difficult to collect and can be prohibitively expensive.
By adopting a combined approach and considering the information and time response needed with the data and knowledge available, it is possible to enhance the effectiveness and efficiency of the risk assessment process, and conform to the organization’s requirements to achieve desired security levels.
Editor’s note: For further insights on this topic, read Volkan Evrin’s recent Journal article, “Risk Assessment and Analysis Methods: Qualitative and Quantitative ,” ISACA Journal , volume 2, 2021.
Don't forget—Members can earn free CPE from ISACA Journal quizzes!
ISACA Now By Year
An Introduction to
Qualitative risk analysis, introduction.
Generally speaking, people aren’t great at analysing risk. Instead of taking a strictly objective view, we’re too easily swayed by our emotions and biases.
Given half a chance most of us will believe what we want to believe and selectively filter out information that doesn’t support our case. We’re just as bad at looking at probability in a holistic way. It’s easy to focus on the most recent risk and forget about one that happened last year.
Availability Heuristic
The tendency to overestimate the likelihood of events with greater ‘availability’ in memory. This can be influenced by how recent the memories are or how unusual or emotionally charged they may be.
Since we’re so bad at considering the big picture when it comes to risk, it makes sense to focus on quantitative risk analysis. Relying on data to determine risk removes bias and ensures accurate assessments. But how do you prioritize those risks? Using qualitative risk analysis.
Qualitative risk analysis is the process of assessing the likelihood of a risk occurring and the impact it would have on a project if it happened.
This guide will walk you through a full breakdown of qualitative risk analysis. You’ll learn:
- The difference between qualitative and quantitative risk analysis
- Types and processes for undertaking an analysis
- Tips and best practices
This will give you insight into the tools and techniques you can use to undertake accurate and cost-effective risk analysis for your projects.
What is Qualitative Risk Analysis?
Qualitative analysis of risk serves 3 functions:
- Prioritise risks according to probability & impact
- Identify the main areas of risk exposure
- Improve understanding of project risks
Projects are exposed to all sorts of risks and it’s impractical for project managers to deal with all of them. In many cases, the resources spent to mitigate a risk actually outweighs the risk itself.
As such, one of the primary goals for qualitative risk analysis is to prioritize risks based on their probability and impact . This allows project managers to focus on devising treatments for the most significant risks.
Using this method also gives project managers a better idea of the main areas of risk exposure. You can achieve this by categorising risks by their source. This is important when it comes to prioritizing risk areas and treatment schedules.
Qualitative risk analysis can also improve a project manager’s understanding of risks. This helps in devising more effective risk treatments and contingency budgeting for future projects. Project managers discover much more than risk probability and consequences. They also discover trigger conditions, assumptions and affected project elements. All of this helps build up a better picture for future projects.
Qualitative vs. Quantitative Risk Analysis
Qualitative risk analysis involves identifying threats (or opportunities), how likely they are to happen, and the potential impacts if they do. The results are typically shown using a Probability/Impact ranking matrix. This type of analysis will also categorize risks, either by source or effect.
Unlike quantitative risk analysis, which applies numerical values and uses verifiable data, qualitative risk analysis operates in a more generalised, “big-picture” space. Quantitative risk analysis uses data to produce a value to measure the acceptability of a risk event outcome.
During a typical project, qualitative risk analysis will happen first. From there, risk managers can draw on data to address specific risks in more detail. So, while they do have two distinctions, they don’t compete for supremacy; they’re two parts of the larger risk management process.
What’s the Difference Between Qualitative and Quantitative Risk Analysis? Click below.

Benefits of Qualitative Risk Analysis
It can be a serious logistical and financial challenge to undertake detailed quantitative modelling necessary for major projects. There are so many factors at play. A qualitative analysis of your risk environment will help give you the clarity to prioritise tasks quickly and cost-effectively.
Other benefits include:
Simple assessment methods
The project team doesn't require training, as it doesn't rely on any complicated tools or software. The qualitative risk analysis doesn’t depend on the risk occurrence frequency. So, the team performing the analysis can save time by not predicting the frequency and the exact timing of each risk. Project teams can determine areas of greater risk in a short time and without expending cost.
Easy prioritisation
Qualitative risk analysis classifies risks according to their likelihood and impact. This makes it easy to determine which risks an organization should focus on – the ones falling into the highest likelihood and impact categories.
Clear presentation options
Limitations of qualitative risk analysis.
Project risk management is a multi-step process. This is because qualitative risk analysis has its limitations. These include:
Subjective Evaluation
A qualitative risk analysis produces no metrics, it depends on the perception of a person carrying out the study. In order to minimise subjectivity, a qualitative risk analysis should involve several people. The accuracy and detail of the analysis depends on previous team experience. If the risk team hasn’t experienced a project type, they might miss some risks or assess them inadequately.
Limited Scope
The qualitative risk analysis assesses each risk on a project but doesn't provide an assessment of the overall project risk exposure. The analysis also won't calculate how much risk management activities and risk treatment will cost.
Lack of Differentiation
Once several risks fall into the same category, for example, high likelihood and medium impact, there is no further way to differentiate between the severity of risks and no way to determine which risk should be dealt with first.
Types of Analysis
Different types of project demand different types of qualitative risk analysis. Availability of resources and personal experience also factor into the decision of how to approach assessing a project’s risk. The five most common types of analysis are:
Probability/Consequence Matrix
- Bow-Tie Analysis
Delphi Technique
Swift analysis, pareto principle.
To many, this is the standard method of establishing risk severity. Risk matrices will often vary in size, but they all essentially do the same thing. They provide a practical way to rank the overall severity of a risk by multiplying the likelihood of risk occurrence against the impact of the risk, should it still occur.
By ranking risk probability against risk consequence, you can see the main driver of risk severity, whether that’s a probability or a consequence. This information helps identify suitable treatments to manage the risk, based on its prominent drivers.
Bow-tie Analysis
A bow-tie analysis is one of the most practical techniques for identifying risk mitigations. Bow-tie analysis starts by looking at a risk event and then projects it in two directions. On the left, you list all the potential causes of an event. On the right, you list all the potential consequences of the event.
Using this simple method, you can identify and apply treatments to each of the causes and consequences separately. This helps you tackle both sides of a risk by mitigating the probability of it occurring one side, while limiting the impact should the risk still occur.
Known as the Delphi Technique, experts in a field respond to several rounds of questionnaires. The responses are aggregated and shared with the group after each round.
When applied to risk management, this technique can be applied to both identify risk, and subsequently to assess the likelihood and impact. The experts are asked to form an opinion on how likely the risk is to occur, and the consequence of its occurrence. These responses are aggregated and reviewed by the experts until a consensus is achieved.
The Delphi technique was conceived in the 1950s by Olaf Helmer and Norman Dalkey of the Rand Corporation. The name refers to the Oracle of Delphi, a priestess at a temple of Apollo in ancient Greece, who was famous for her prophecies.
Standing for “Structured What-If Technique”, SWIFT applies a systematic, team-based approach to risk analysis in a workshop environment. Teams investigate how changes from an approved plan, may affect a project through a series of “What if” considerations. This technique is particularly useful in evaluating the viability of opportunity risks.
Better known as the "80/20 Rule", the Pareto Principle helps in identifying risks that will be most effective. It's known as 80/20 because the principle thesis holds that 80% of achievements realised originate from 20% of the effort.
Risk managers use Pareto analysis as a tool for rapidly identifying the most critical 20% of risks that will effectively mitigate 80% of the impact.
The challenge for risk managers is knowing how to effectively score each risk. Large projects may require multi-attribute weightings for business different priorities, such as security data, and operational or compliance policies.
But, once you understand where to look and what to look at will help you hone in on the most important 20%. This offers a crucial leg up in managing the threats and vulnerabilities that have the potential to have the largest impact.
Qualitative Risk Analysis Process
Like any big task that's worth doing, risk management can seem daunting - especially when you're starting with a blank canvas. So, the best way to take on qualitative risk analysis is to break it down into smaller steps:
- Identifying Risks
- Impact Analysis
- Risk Treatment
- Review & Monitor
1. Identifying Risks
Risk identification is arguably the most important part of qualitative risk analysis. If you fail to identify risks ahead of time, it becomes extremely challenging to manage them.
The trick to risk identification is keeping it simple. Start thinking of anything which could have an uncertain effect on your project. Capturing the obvious risks will help lead you deeper into more oblique ones. Risk identification is all about quantity. So, reach out to as many people as you can to get a wide range of views.
Tools for Risk Identification
- Questionnaires
- Documentation review
- Checklist analysis
- SWOT Analysis
2. Impact Analysis
Once you’ve identified possible risks, the next step is to consider their potential impact.
- Segregate the risks into threats and opportunities, but remember that they are similar but not opposite .
- Using qualitative risk analysis, estimate the impact of each risk on a scale (1-5 or low/medium/high/extreme).
- Next, estimate the probability of each risk occurring, using a similar scale.
- Finally, take those scores and combine them to create a total risk ranking.
Simplicity is the major benefit of qualitative risk analysis; there’s no statistical model that relies heavily on the quality of the data you use.
3. Risk Treatment
The next stage in the qualitative risk analysis is to apply treatments to each risk. This can be approached in any number of ways depending on your industry or process. A simple example could show five options when it comes to risk treatment, but these are by no means definitive:
If a risk has low impact and low probability, or the cost of preventing it is too high, sometimes it’s more cost-effective to accept it.
Some risks have a high probability, which means you might not be able to avoid them. In order to reduce the impact of a risk when it becomes an issue, you could choose to mitigate it.
A few risks can be exploited to the benefit of your project. Having the ability to identify exploitable risks can be extremely advantageous and highlights the importance of seeking out experienced risk experts who can spot these opportunities.
Risks with financial impacts are a common example of risks that can be transferred to a third party. Insurance is designed to assume a risk on your behalf, so you don’t suffer as hard an impact if something goes wrong. Similarly, it is possible to transfer risk via a contract to a supplier or contractor.
If you can’t mitigate or transfer a risk, and that risk is too high to accept, the only recourse is to avoid it. Risks can be avoided by changing or removing certain scope items or changing the approach.
Contingency Planning
If a risk becomes an issue, you need a plan. You need to know:
- who gets notified
- who does what
Documenting a contingency plan saves time and money. When you know what to do in the event of an issue, you can reduce its impact by responding faster. The nature and detail of your contingency planning will depend on the nature of the risks themselves.
4. Review & Monitor
Risk management is never over, not even after the project has finished. As the project progresses, it’s important to keep risk logs up to date. At each stage of the project, risk probability will fluctuate. Some risks will disappear, while others might increase in likelihood. Reviewing your risks regularly will help keep you on top of these changes.
After the project, a full retrospective will provide valuable data and experience for future projects, making the next one more secure and helping to further your risk maturity.
Risk Appetite
The risk matrix can be used to set the risk appetite for the organisation. The simple use of colour can aid the decision-making process as well helping to set the risk culture across the group. A risk hungry company may have a large tolerance for taking risk, whereas a high-risk company, for example in the nuclear industry, may set their appetite a lot lower.
In the example, all risks in the red area are intolerable and must be treated to reduce them to acceptable levels.
Risk matrices should be used for subjective guidance, not to provide you with definitive quantitative risk ranking data.
Risk Escalation
What happens when a risk goes from Yellow to Red? Does the risk owner still have the authority to manage the risk effectively, or should it be escalated?
If the risk owner has the tools to manage that risk, there's no need to escalate. Simply maintain a clear line of communication on the progress of bringing the risk down to an acceptable level and there's no need for escalated action.
Why should you escalate?
- If there's absolutely nothing you can do to bring the risk down to an acceptable level.
- If treatment requires action outside the delegation of the original risk.
- If you're managing a shared risk.
Risk management is all about the creation of a culture in which decisions are made based on the assessment of data in order to maximise opportunity and minimise the consequence of threats.
Qualitative risk management is a key component in the risk professionals’ tool kit. It enables rapid prioritisation of risks to help project teams to achieve their objectives. Through using these techniques your project will have a greater chance of being delivered on time and within budget.
Experience Safran Risk Manager

About Safran
Since 1997, we have worked closely with our customers to understand the complex requirements of planning and project controls software. This close relationship and process of continuous improvement means our latest software addresses the needs of the 21st century risk environment.
We pride ourselves in offering outstanding support to all our customers. Our team of project management and planning professionals are dedicated to helping you achieve your project goals.
Safran software is used to control some of the world’s most complex projects across industries including:
- oil and gas
- engineering
- construction
- aerospace and defence
- public sector
We understand the strict requirements for stability, performance, and scalability in modern projects and design our software accordingly.
Designed to support contingency management and identify impacts of risk, Safran Risk Manager helps you make better strategic decisions. Whether you're tackling a complex capital project, managing a turnaround, or planning operational maintenance, our integrated project management tools make life easier.
Planview Blog
Your path to business agility
The Best Qualitative Risk Assessment Methods
A defining skill set of any effective project manager is their ability to assess and mitigate risk. Spotting bumps in the road, predicting outcomes and preventing failures are all part of the responsibility of managing a project successfully.

Risk assessment can be an art form , and there’s a variety of ways to get the job done. We’ll provide a basic rundown below.
What is Risk Assessment?
The broad definition of managing risk is the ability to identify and define any risk(s) associated with a decision, then evaluate all possible outcomes and potential impacts of said risk. It’s the capacity to see problems as they arise, deal with them when they do and, finally, try to prevent them from happening again.
There are two types of risk assessment: qualitative and quantitative. Qualitative risk assessment methods are the most effective but are typically difficult to fund due to their lack of numerical estimates. In qualitative management, descriptive and categorical treatments of information are used in lieu of quantitative estimates. They are analytical, evidence-based characterizations of risk, but still provide two primary functions:
- Identification of risk
- Risk characterization and analysis
Importance and Elements of the Risk Narrative
A risk narrative is the starting point for any healthy assessment. The risk narrative is simply a way to identify and depict a specific risk. It includes a description of the four generic risk assessment types:
- Categorizing hazard
- Consequences
The risk narrative is where the problems get identified, defined and described. Of course, that’s only half the battle – the rest consists of actually assessing that information. When it comes to analyzing the narrative, there are a multitude of qualitative risk assessment methods one can use. We’ll explore some below.
Methods for Risk Analysis
In the same way that there isn’t a universal method to measuring temperature, there’s also a wide range of ways to qualitatively assess risk. The following are just a few of the most popular methods.
Risk Probability and Impact Assessment
This method involves looking into the likelihood of each risk and the ways it may affect separate project objectives , such as those tied to budget, schedule and performance. In this case, negative effects are “threats” and positive effects are “opportunities.”
This type of assessment is generally performed through meeting and interviewing stakeholders, investigating ongoing work and thoroughly documenting results. The PM can then define the threats and opportunities on varying levels depending on how they will affect the project.
Qualitative Risk Assessment Matrix (RAM)
A probability and impact matrix is the first step to defining the rating scales for likelihood and impact of a particular risk. Ratings rules should be specified by the organization in advance so that the project manager knows what to prioritize.
The ultimate goal of the matrix is to identify which risks you need to develop a response for. Likelihood and impact are typically rated on the following scale:
These scales are highly dependent on the specs of the project. Therefore, the project manager must perform a matrix for each individual task.
Risk Categorization
Grouping risks by their common causes can aid in sorting and prioritizing the problems. It helps to determine the areas of the projects that are most exposed to risk and work backwards from there. Categorizing risks allows project managers to view them in smaller, easy-to-manage groups—much like breaking up the tasks in a project .
Urgency Assessment
In qualitative risk analysis, the impending threat of the risk itself must be taken into consideration. The risk ranking determined from the probability matrix combined with the risk urgency can give a project manager a final risk sensitivity rating that can help them better prioritize and manage projects.
Professional Opinion
The judgment of an expert in the field should never be overlooked. Interviews and risk facilitation workshops are just two ways in which you can connect with professionals on managing qualitative risk assessment.
Assessing risk is almost like predicting the future—it’s not an exact science. But with the proper tools – like those from Planview AdaptiveWork – qualitative measures and an open mind, a skilled project manager will be able to avoid risk and continuously steer their projects to success.

Related Posts


An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
Risk to researchers in qualitative research on sensitive topics: issues and strategies
Affiliation.
- 1 School of Public Health, La Trobe University, Bendigo, Victoria, Australia. [email protected]
- PMID: 18174541
- DOI: 10.1177/1049732307309007
Traditionally, risk assessments in research have been limited to examining the risks to the research participants. Although doing so is appropriate and important, there is growing recognition that undertaking research can pose risks to researchers as well. A grounded theory study involving a range of researchers who had undertaken qualitative health research on a sensitive topic was completed. Analysis of the in-depth, face-to-face unstructured individual interviews with 30 Australian public health researchers provided evidence that researchers do confront a number of physical and emotional risks when undertaking research. Training, preparation, and supervision must be taken into account so that the risk to researchers can be minimized. Researchers need to consider occupational health and safety issues in designing research projects that deal with physical and emotional risks. Recommendations for professional supervision, policy development, and minimum training standards for researchers are provided.
PubMed Disclaimer
Similar articles
- Blurring boundaries in qualitative health research on sensitive topics. Dickson-Swift V, James EL, Kippen S, Liamputtong P. Dickson-Swift V, et al. Qual Health Res. 2006 Jul;16(6):853-71. doi: 10.1177/1049732306287526. Qual Health Res. 2006. PMID: 16760540
- Keeping nurse researchers safe: workplace health and safety issues. Barr J, Welch A. Barr J, et al. J Adv Nurs. 2012 Jul;68(7):1538-45. doi: 10.1111/j.1365-2648.2012.05942.x. Epub 2012 Feb 7. J Adv Nurs. 2012. PMID: 22309294
- Perceptions about safety and risks in gender-based violence research: implications for the ethics review process. Sikweyiya Y, Jewkes R. Sikweyiya Y, et al. Cult Health Sex. 2011 Oct;13(9):1091-102. doi: 10.1080/13691058.2011.604429. Epub 2011 Aug 9. Cult Health Sex. 2011. PMID: 21824018
- Risks of alcohol consumption in laboratory studies involving human research participants. Wood MD, Sher KJ. Wood MD, et al. Psychol Addict Behav. 2000 Dec;14(4):328-34. Psychol Addict Behav. 2000. PMID: 11130151 Review.
- Telephone focus groups in physiotherapy research: potential uses and recommendations. Smith JM, Sullivan SJ, Baxter GD. Smith JM, et al. Physiother Theory Pract. 2009 May;25(4):241-56. doi: 10.1080/09593980902782496. Physiother Theory Pract. 2009. PMID: 19418362 Review.
- Considering Risks to Researchers and Staff in Low-Resource Settings during Public Health Crises: A Proposed Conceptual Model. Perez KM, Asim M, Weiss EM, Valentine GC, Kavi A, Somannavar MS, Iwuh I, Chiweza C, Tickell KD, Singa BO, Beima-Sofie K, Batra M, Walson JL, Umoren R, Kelley M, Saleem S. Perez KM, et al. Children (Basel). 2023 Feb 26;10(3):463. doi: 10.3390/children10030463. Children (Basel). 2023. PMID: 36980021 Free PMC article.
- Researching Alcohol Consumption During Pregnancy. Opportunities and Challenges With Two Methods of Data Acquisition. Binder A, Preiser C, Hanke S, Banabak M, Huber C, Petersen KU, Batra A. Binder A, et al. Qual Health Res. 2022 Oct;32(12):1809-1827. doi: 10.1177/10497323221119005. Epub 2022 Aug 25. Qual Health Res. 2022. PMID: 36017584 Free PMC article.
- Women Caring for Husbands Living with Parkinson's Disease: A Phenomenological Study Protocol. White DR, Palmieri PA. White DR, et al. J Pers Med. 2022 Apr 20;12(5):659. doi: 10.3390/jpm12050659. J Pers Med. 2022. PMID: 35629082 Free PMC article.
- Opening the Black Box of Daily Life in Nonsuicidal Self-injury Research: With Great Opportunity Comes Great Responsibility. Kiekens G, Robinson K, Tatnell R, Kirtley OJ. Kiekens G, et al. JMIR Ment Health. 2021 Nov 19;8(11):e30915. doi: 10.2196/30915. JMIR Ment Health. 2021. PMID: 34807835 Free PMC article.
- Development and evaluation of guidelines for prevention of retraumatisation in torture survivors during surgical care: protocol for a multistage qualitative study. Schippert AC, Grov EK, Dahl-Michelsen T, Silvola J, Sparboe-Nilsen B, Danielsen SO, Aaland M, Bjørnnes AK. Schippert AC, et al. BMJ Open. 2021 Nov 5;11(11):e053670. doi: 10.1136/bmjopen-2021-053670. BMJ Open. 2021. PMID: 34740935 Free PMC article.
- Search in MeSH
LinkOut - more resources
Full text sources.

- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
- +1 (800) 826-0777
- VIRTUAL TOUR
- Mass Notification
- Threat Intelligence
- Employee Safety Monitoring
- Travel Risk Management
- Emergency Preparedness
- Remote Workforce
- Location and Asset Protection
- Critical Communication
- Business Continuity
- Why AlertMedia
- Who We Serve
- Customer Spotlights
- Resource Library
- Downloads & Guides

Qualitative Risk Analysis & Other Types of Risk Assessment
Choosing the right risk assessment methodology, whether qualitative, quantitative, or both, is crucial for effectively managing threats.

- Risk Identification and Responses
Qualitative Risk Analysis
Quantitative risk evaluation, semi-qualitative risk assessment tools.
“Research the threat and apply data from sources like public records, social media, dark net—so that you can learn as much as possible.” Lukas Quanstrom Co-Founder and CEO, Ontic
When is a threatening letter to a business more than an empty threat? How do you determine when it becomes a genuine risk? Lukas Quanstrom , co-founder and CEO at Ontic, regularly confronts these challenges. In a recent interview on The Employee Safety Podcast , Quanstrom shared how understanding the severity of such threats requires more than surface-level analysis. It requires a detailed, strategic, and proactive approach.
“Once a potential threat has been identified, the next step is to research the threat and apply data from sources like public records, social media, dark net—so that you can learn as much as possible,” Quanstrom said. Research and assessment are critical to understanding how to manage business threats, and there are a few different risk assessment methodologies, each with its strengths and formats.
These strategies range from a qualitative risk analysis that relies on expert judgment and scenario analysis to quantitative methods that use statistical data and mathematical models. Some methodologies even sit squarely in the middle, using descriptions and data to establish a risk management program. Picking the correct method will help you manage threats against your business by providing a structure to understand the likelihood and impact of those threats.
Download Our Operational Risk Assessment Template
Risk identification and risk responses.
When assessing risks, it’s essential to recognize that various types of risks can affect a business. This article will focus on four key categories of risk: strategic, compliance, financial, and operational risk . But it’s important to remember that these are just a few examples of the broad range of risks businesses may encounter.
| Risks arising from adverse business decisions, poor implementation, or a lack of responsiveness to industry changes. (e.g., a new competitor enters the market) | Risks related to legal requirements, regulations, or internal policies—which can lead to legal penalties, financial forfeiture, and reputational damage. (e.g., a new privacy law is introduced) | Risks involving potential financial losses due to market fluctuations, credit risk, liquidity issues, and investments. (e.g., interest rates rise on a business loan) | Risks from failures in processes, people, systems, or . (e.g., a cybersecurity incident takes out company networks and infrastructure) |
A practical risk assessment aims to better understand how to manage those risks. These are the four primary risk management responses:
- Avoidance: Eliminating the risk
- Mitigation: Reducing the impact or likelihood of the risk event
- Transfer: Shifting the risk to another party, such as through insurance
- Acceptance: Acknowledging the risk and choosing to deal with its potential consequences
Your chosen risk assessment methodologies will help you understand the threats your business faces and choose from one of the above options for handling them. With thorough analysis, you can make informed decisions that align with your organization’s risk tolerance and strategic goals.
3 Risk Assessment Methodologies
The steps of a risk assessment are relatively straightforward: identify threats, assess those threats, develop controls, and evaluate your response.

However, these four steps leave much room for interpretation—and error. A risk assessment methodology is a systematic approach underlying all four stages by qualifying or quantifying the threat. That is why most risk assessments use one of these three methodologies:
- Qualitative: Determining risks based on subjective judgment and descriptive measures rather than numerical data or statistics.
- Quantitative: Evaluating risks by estimating specific threats’ probability and potential impact using numerical data and statistical methods.
- Semi-Qualitative: Combining aspects of both qualitative and quantitative analysis.

Qualitative vs. quantitative risk analysis, with a blended assessment option
Qualitative risk assessments are a type of risk evaluation that relies on subjective judgment and expert opinions rather than numerical data. This methodology is beneficial when data is unavailable, incomplete, or difficult to quantify. Qualitative risk assessments often involve identifying potential risks through brainstorming sessions, expert interviews, and workshops. These assessments rely on scenarios and descriptive analysis to evaluate the likelihood of occurrence and impact of risks.
One key benefit of qualitative risk assessments is their flexibility. They can be tailored to fit a business’s needs and context, making them highly adaptable to various industries and situations. Unlike quantitative assessment methods, which require detailed data and statistical models, you can perform a qualitative risk analysis with limited information and still consider a broad range of risks.
Another benefit is their ability to incorporate the insights and expertise of individuals who may deeply understand potential risks but lack access to comprehensive data. This subjective approach can provide valuable context and nuance that quantitative methods might overlook.
Numerous customized qualitative risk assessment models are available, with several well-established methodologies, such as those from the International Organization for Standardization (ISO), gaining widespread recognition for their effectiveness. These methodologies offer structured approaches to identifying and analyzing risks based on expert judgment and descriptive analysis.
ISO 27001 is a qualitative strategy typically associated with cybersecurity, but its influence can extend into other domains. It is tailored to establish, implement, maintain, and continuously improve information security management systems (ISMS) to safeguard sensitive information.
This widely recognized qualitative risk assessment methodology is primarily associated with cybersecurity, though you can apply its principles across various domains. This standard provides a structured approach for establishing, implementing, maintaining, and continuously improving an Information Security Management System (ISMS) to protect sensitive information.
An ISO 27001 assessment focuses on three critical areas—people, processes, and technology.
- People: This involves assessing risks related to employees and other individuals with sensitive information access. It includes evaluating the effectiveness of training programs, identifying potential insider threats, and ensuring that roles and responsibilities for information security are clearly defined and communicated.
- Processes: This area focuses on evaluating and improving the procedures and policies to manage information security. It includes reviewing existing security policies, conducting risk assessments, and implementing controls to address identified risks. Regular audits and reviews are part of this process to ensure that procedures remain effective and are updated as needed.
- Technology: This involves assessing the technical controls and systems that protect sensitive data. It includes evaluating the security of IT infrastructure, software, and hardware and then implementing measures such as encryption, access controls, and monitoring systems to prevent and respond to security incidents.
By addressing these three critical areas, ISO 27001 helps organizations systematically identify, mitigate, and manage risks to information security.
Decision trees
A decision tree is a dynamic risk assessment tool that uses a diagrammatic approach to map out possible outcomes and their associated risks for decision-making. Seeing a visual representation of the flow can often help stakeholders understand the potential consequences of each decision branch.
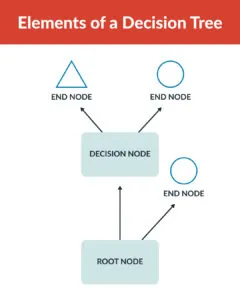
As the diagram above shows, decision trees have three components: the root, the decisions, and the endpoints.
- Root: The root of a decision tree represents the starting point or initial decision that needs to be made.
- Decisions: Decision nodes are points within the decision tree where choices or alternatives are considered. Each decision node branches out into one or more possible outcomes or actions that can be taken based on the decision made at that point.
- Endpoints: These are the outcomes or results of following a specific path through the decision tree. They represent the consequences or outcomes of the decisions made at each preceding node.
You can apply many qualitative methodologies to improve risk assessments, but they’re not always ideal because they lack precision and quantifiable metrics. While qualitative approaches provide valuable insights into subjective factors such as organizational culture and human behavior, they may struggle to deliver measurable and comparable data points for rigorous analysis and decision-making. This is where semi-qualitative risk assessment methodologies become invaluable.
Quantitative risk assessments involve assigning numerical values to potential threats, allowing organizations to evaluate the likelihood of risks, predict their impacts, and estimate potential losses. This data-driven approach provides a precise measurement of risk, which can be invaluable for businesses looking to make informed decisions based on empirical evidence.
A business chooses this risk assessment approach for a few different reasons. Some of the significant benefits of a quantitative risk assessment are:
- Increased accuracy: Quantitative risk assessments provide precise numerical data, which helps businesses measure risk more accurately than qualitative methods that rely on subjective judgment.
- Enhanced objectivity: Quantitative assessments minimize personal biases with statistical data and mathematical models, offering a more objective risk evaluation than qualitative approaches.
- Improved comparability: Quantitative data allows for direct comparison between different risks, which is often more challenging with qualitative assessments that may use descriptive or subjective criteria.
- Better forecasting: Quantitative methods use historical data to predict future risk scenarios, offering more reliable forecasting capabilities than qualitative methods that may not use historical data as effectively.
- Clear communication: Quantitative results provide concrete numbers that can be easier to communicate and justify to stakeholders, as opposed to qualitative descriptions that might be more open to interpretation.
- Benchmarking and performance measurement: Quantitative data enables benchmarking against industry standards and measuring performance over time, which qualitative methods may not directly support.
One standard quantitative risk methodology involves using historical weather data and statistical models to predict the probability of a hurricane occurring in a specific area. Meteorologists might analyze past hurricane patterns, sea surface temperatures, and atmospheric conditions to calculate the likelihood of a hurricane’s landfall in a given region over the next year. They pass this information on to businesses that use quantitative data to manage the risk.
Businesses in vulnerable areas can prioritize risks and management efforts by assigning numerical probabilities to different levels of hurricane risk. For example, a company operating in a region with a high probability of hurricanes might invest in enhanced building infrastructure and emergency response plans. At the same time, a business in a lower-risk area might allocate fewer resources to hurricane preparedness. This data-driven approach allows for targeted risk mitigation strategies based on quantified risk probabilities.
Another example of quantitative risk assessment involves using financial models to predict the effects of changes in interest rates on a company’s bottom line. A company with significant debt might use historical interest rate data and financial modeling techniques to estimate how fluctuations in interest rates could impact its interest expenses and overall profitability.
The company can project potential financial outcomes under different interest rate scenarios by applying quantitative methods, such as sensitivity analysis or scenario modeling. For example, if interest rates are predicted to rise by 1%, the company can estimate the increase in interest payments and its effect on net income. These insights allow the business to make informed decisions about financial strategies, such as refinancing debt or adjusting investment plans, based on numerical projections of potential impacts.
Semi-qualitative risk assessment methodologies combine the precision of quantitative data with the depth of qualitative analysis, offering a thorough and rigorous approach to understanding risks. This method leverages numerical data to provide concrete risk probability and impact estimates while incorporating qualitative insights to capture nuances that numbers alone may not reveal.
Semi-qualitative assessments enable organizations to examine risks from multiple angles by integrating data-driven and judgment-based perspectives. This comprehensive approach ensures that potential threats are evaluated in terms of statistical likelihood while considering contextual implications and expert opinions.
This combined approach results in a more complete risk profile, facilitating better-informed decision-making. Organizations benefit from a detailed understanding of risks, allowing them to develop strategies that address both the measurable and less quantifiable aspects of potential threats.
Risk matrix
A risk matrix is the most straightforward semi-qualitative approach. This tool categorizes direct risks based on their likelihood and potential impact, as depicted below.

Using a risk matrix enables efficient risk management through hazard identification and categorization. The tool weighs risks based on their likelihood and impact, visually presenting the severity of each risk scenario. Using a risk matrix—especially along with a risk register —organizations can prioritize resources and efforts toward mitigating significant, high risks while effectively communicating the rationale behind risk management decisions to key stakeholders.
Suppose the risk matrix is a straightforward example of a semi-qualitative methodology. In that case, an integrated threat intelligence system represents the opposite end of the spectrum with more detailed analysis.
Integrated threat intelligence system
Threat intelligence systems gather and analyze comprehensive information about potential hazards, aiding organizations in proactive risk mitigation and response strategies. They can also be critical tools for assessing and understanding your specific risks. In his interview, Lukas Quanstrom also highlighted the evolving role of threat intelligence in proactive corporate security risk assessment. Quanstrom emphasized that traditional reactive threat management is giving way to a more proactive approach enabled by what he terms “protective intelligence.”
Protective intelligence integrates investigative (qualitative) techniques with advanced analytics (quantitative) to detect and assess potential threats early on. These indicators, such as threatening communications or unusual patterns in employee behaviors, serve as early warning signals that enable proactive risk mitigation strategies . Using data to define a threat’s likelihood and impact allows organizations to prioritize strategies.
Quanstrom explained, “By adopting a proactive, always-on security approach, you can continually collect and connect pre-incident physical threat indicators, providing the critical knowledge needed to prevent bad things from happening.” This proactive stance safeguards assets and personnel, supports business continuity, and enhances stakeholder confidence in the organization’s resilience to emerging threats.
Combining Risk Analysis Processes
Qualitative, quantitative, and semi-qualitative risk assessment methodologies have strengths and limitations. Integrating all three of these approaches offers you a more comprehensive risk assessment so you better understand your potential threats and vulnerabilities. With that situational awareness, you can make informed decisions and prioritize resources where they are most needed.
By combining qualitative insights with quantitative data and semi-qualitative assessments, businesses can establish a dynamic risk management plan that adapts to identified risks and enhances overall resilience.
More Articles You May Be Interested In

Operational Risk Assessment Template
Please complete the form below to receive this resource.
Check Your Inbox!
The document you requested has been sent to your provided email address.
Cookies are required to play this video.
Click the blue shield icon on the bottom left of your screen to edit your cookie preferences.

The Essex website uses cookies. By continuing to browse the site you are consenting to their use. Please visit our cookie policy to find out which cookies we use and why. View cookie policy.
Research risk assessment
It's the responsibility of the principal investigators (PI) and researchers to identify reasonably foreseeable risks associated with their research and control the risks so far as is reasonably practicable.
All participants and research assistants have the right to expect protection from physical, psychological, social, legal and economic harm at all times during an investigation. Certain research may also present reputational, legal and / or economic risks to the University.
As part of the ethical approval process for research involving human participants you are required to identify potential risks associated with your research and the action you will take to mitigate risk. You may be asked to submit your risk assessment.
The risk assessment process is a careful examination of what could cause harm, who/what could be harmed and how. It will help you to determine what risk control measures are needed and whether you are doing enough.
Risk assessment responsibility
The PI and researchers need to take responsibility for all assessments associated with their projects. Occasionally you may need research workers or students to risk assess an aspect of the work and you will need to check the assessments are adequate and sign them off.
Risk assessors need to be competent and you’ll need to ensure they have adequate training and resource to do the assessments. There is risk assessment training available and help and advice help and advice help and advice from your Health and Safety adviser and safety specialists (for health and safety risks), or the REO Research Governance team for other risks. In some cases, the hazards are so unique to the research that the PI and their team might be the only people who know the work well enough to make valid judgements about the risk and justify their conclusions.
Risk assessment process
The risk assessment process is a careful examination of what could cause harm, who/what could be harmed and how. It will help you to determine what risk control measures are needed and whether you are doing enough.
To simplify the process you can use the health and safety risk assessment templates, risk estimation tool and guidance for all risks associated with your research project. Please refer to the research risk estimation guidance under how to carry out a risk assessment below to assist you.
Research risks
Typical risks that need to be considered as part of research ethics are:
- Social risks: disclosures that could affect participants standing in the community, in their family, and their job.
- Legal risks: activities that could result in the participant, researchers and / or University committing an offence; activities that might lead to a participant disclosing criminal activity to a researcher which would necessitate reporting to enforcement authorities; activities that could result in a civil claim for compensation.
- Economic harm: financial harm to participant, researcher and / or University through disclosure or other event.
- Reputational risk: damage to public perception of University or the University/researchers’ reputation in the eyes of funders, the research community and / or the general public.
- Safeguarding risks: Risk to young people, vulnerable adults and / or researcher from improper behaviour, abuse or exploitation. Risk to researcher of being in a comprising situation, in which there might be accusations of improper behaviour.
- Health and safety risks: risks of harm to health, physical injury or psychological harm to participants or the researcher. Further information on health and safety risks is given below.
Health and safety risks
The potential hazards and risks in research can be many and varied. You will need to be competent and familiar with the work or know where to obtain expert advice to ensure you have identified reasonably foreseeable risks. Here are some common research hazards and risks:
- Location hazards Location hazards Location hazards and risks are associated with where the research is carried out. For example: fire; visiting or working in participant’s homes; working in remote locations and in high crime areas; overseas travel; hot, cold or extreme weather conditions; working on or by water. Also hazardous work locations, such as construction sites, confined spaces, roofs or laboratories. For overseas travel, you will need to check country / city specific information, travel health requirements and consider emergency arrangements as part of your research planning, by following the University’s overseas travel health and safety standard .
- Activity hazards Activity hazards Activity hazards and risks associated with the tasks carried out. For example: potentially mentally harmful activities; distressing and stressful work and content; driving; tripping, or slipping; falling from height; physically demanding work; lifting, carrying, pushing and pulling loads; night time and weekend working.
- Machinery and equipment Machinery and equipment Machinery and equipment . For example: ergonomic hazards, including computer workstations and equipment; contact with electricity; contact with moving, rotating, ejecting or cutting parts in machinery and instruments; accidental release of energy from machines and instruments.
- Chemicals and other hazardous substances . The use, production, storage, waste, transportation and accidental release of chemicals and hazardous substances; flammable, dangerous and explosive substances; asphyxiating gases; allergens; biological agents, blood and blood products. You’ll need to gather information about the amount, frequency and duration of exposure and carry out a COSHH or DSEAR assessment which will inform whether you may need health surveillance for yourself and / or your research participants.
- Physical agents Physical agents Physical agents . For example: excessive noise exposure, hand-arm vibration and whole body vibration; ionising radiation; lasers; artificial optical radiation and electromagnetic fields. You’ll need to gather information about the amount, frequency and duration of exposure inform whether you may need health surveillance for yourself and / or your research participants.
When to carry out a risk assessment
Carrying out initial risk assessments as part of the planning process will help you identify whether existing resources and facilities are adequate to ensure risk control, or if the project needs to be altered accordingly. It will also help you to identify potential costs that need to be considered as part of the funding bid.
Once the project is approved, research specific risk assessments need to be carried out before work starts.
The research may need ethical approval if there is significant risk to participants, researchers or the University.
How to carry out a risk assessment
The University standard on risk assessments provides guidance, tips on getting it right, as well as resources and the forms to help you produce suitable and sufficient risk assessments and must be used.
- Risk assessment template (.dotx)
- Flow chart to research risk assessment (.pdf)
- Research risk assessment: Risk estimation tool (.pdf)
- Example of a Social Science research risk assessment (.pdf)
Refer to carrying out a risk assessment carrying out a risk assessment carrying out a risk assessment for step by step guidance.
Risk assessments must relate to the actual work and must be monitored by the PI. If there are significant changes to the activities, locations, equipment or substances used, the risk assessment will need to reviewed, updated and the old version archived. Risk assessments should also consider the end of projects, arrangements for waste disposal, equipment, controlled area decommission and emergencies.
Things to consider:
- The risks may be specialist in nature or general. Information can found from legislation, sector guidance, safety data sheets, manufacturers equipment information, research documents, forums and health and safety professionals.
- Practical research might involve less well-known hazards. Do you or your team have the expertise to assess the risk adequately? Do you know who to go to for expert advice?
- The capabilities, training, knowledge, skills and experience of the project team members. Are they competent or are there gaps?
- In fast changing research environments, is there a need to carry out dynamic risk assessments? Are they understood and recorded?
- The right personal protective equipment for the hazards identified and training in how to use it.
- Specific Occupational Health vaccinations, health surveillance and screening requirements identified and undertaken. With physical agents and substances you’ll need to make an informed decision about the amount, frequency and duration of exposure. If you need help with this contact Health and Safety.
- Associated activities: storage, transport/travel, cleaning, maintenance, foreseeable emergencies (eg spillages), decommissioning and disposal.
- The safe design, testing and maintenance of the facilities and equipment.
- Planned and preventative maintenance of general plant and specialist equipment.
These risk assessments relate to the actual work and must be monitored by the PI. If there are significant changes to the activities, locations, equipment or substances used, the risk assessment will need to reviewed, updated and the old version archived. Risk assessments should also consider the end of projects, arrangements for waste disposal, equipment and controlled area decommission and emergencies.
Training
If you would like training on completing a risk assessment, please book onto our Risk Assessment Essentials course via HR Organiser. If you are unable to access this, please email [email protected]
- Carrying out a risk assessment Carrying out a risk assessment Carrying out a risk assessment
- People especially at risk People especially at risk People especially at risk
- IOSH/USHA/UCEA guidance on managing health and safety in research (.pdf)
- Research governance: Ethical approval
- For enquiries contact your Student Services Hub
- University of Essex
- Wivenhoe Park
- Colchester CO4 3SQ
- Accessibility
- Privacy and Cookie Policy
- Sign up for free
- SafetyCulture
Qualitative and Quantitative Risk Analysis
Learn more about qualitative and quantitative risk analysis. Discover how these methods help organizations address risks and hazards.

What is Qualitative Risk Analysis?
Qualitative risk analysis is the process of evaluating and rating an identified risk based on its severity and the likelihood of its consequences. The goal of qualitative risk analysis is to come up with a short list of risks that need to be prioritized above others.
Qualitative risk analysis is best described as a project manager ’s first line of defense against risks. It helps weed out potential detractors to the project’s success, including risks that are unlikely to cause any severe harm to the project. By targeting the most dangerous risks first, risk analysis in project management becomes more efficient and project managers are able to allocate their time and resources more effectively.
What is Quantitative Risk Analysis?
As part of the overall quantitative risk management process, quantitative risk analysis is the process of calculating risk based on data gathered. The goal of quantitative risk analysis is to further specify how much will the impact of the risk cost the business. This is achieved by using what’s already known to predict or estimate an outcome.
For data to be suitable for quantitative risk analysis, it has to have been studied for a long period of time or to have been observed in multiple situations. For example, in the past five projects, equipment type A has broken down after 7 hours of use. With this information, it can be assumed that if a project requires workers to use equipment type A for 8 hours, then it has a 100% chance of breaking down.
Difference Between Qualitative and Quantitative Risk Analysis
The key difference between qualitative and quantitative risk analysis is the basis for evaluating risks. As mentioned earlier, qualitative risk analysis is based on a person’s perception or judgment while quantitative risk analysis is based on verified and specific data.
Another difference is the values associated with risks. In qualitative risk analysis, this value is the risk rating or scoring. A risk may be rated “Low” or given a score of 1 to indicate that the risk does not require immediate attention. In quantitative risk analysis, the value associated with the risk is often in percentages and indicates the probability of the risk occurring or of it causing a specific negative effect on project objectives.
To help guide project managers in selecting which risk analysis to perform, here are examples of instances where a qualitative or quantitative risk analysis may be applied.
Examples of Qualitative Risks/Problems
Change in perception of a risk – Example: The lack of machine guards was initially given a risk rating of low, but after several near misses involving the hazard occurred, the project manager believes its risk rating should be at least medium.
New risk has been identified – Example: When the project began, equipment was in good condition. The only risk the project manager could identify at the time was the lack of proper training , as most of the workers did not know how to use equipment safely. The project manager quickly arranged for the workers to be trained in equipment safety . Yet, as the workers started to use equipment more frequently, the project manager noticed that it was no longer in good condition and could malfunction soon.
Examples of Quantitative Risks/Problems
Large amount of data on the risk and its impact – Example: In 2020, a construction company planned on starting a major project in 2021. In preparation for the project , the construction company began collecting data on the risks they may face, their impact on the project’s completion, and how much mitigating these risks could cost the company. By early 2021, the construction company had enough data to perform a quantitative risk analysis.
Qualitative risk analysis needs to be validated – Example: During qualitative risk analysis, a project manager scored each risk a 10 on a scale of 1-10, with 10 being extremely high risk. But the project manager wants to ensure that each risk has an impact great enough to justify spending time and resources on them.
How to Perform Qualitative and Quantitative Risk Analysis
After choosing which risk analysis best fits their given situation, project managers can proceed with performing the risk analysis. For those looking for a guide on how to perform qualitative and quantitative risk analyses, follow the steps below:
Qualitative Risk Analysis Steps
Step 1: identify risks.
The goal of this step is to create a masterlist of risks by noting down any risk that comes to mind and asking other members of the team for their input. Additionally, project managers can make the risk identification process faster by holding brainstorming sessions with their teams and even some workers to get a clearer idea of what’s happening in the field.
Step 2: Classify Risks
There are several techniques for classifying risks. One popular technique is the risk matrix, which combines the consequences and likelihood of a risk occurring.

Risk Matrix
Lesser known techniques include assessing the possible causes and effects of each risk and preparing for different scenarios involving the risk.
Step 3: Control Risks
While this may look different depending on the technique chosen in the previous step, risk control is generally divided into two categories. The first category of risk control is focused on targeting the root causes of risks such as hazards or inefficient management processes. The second category of risk control is geared towards lessening the negative impact of the risk through corrective actions such as providing workers with PPE .
Step 4: Monitor Business Risks
As project managers go through the qualitative risk analysis process, they should remember to keep all of their notes regarding risks, risk ratings, and control measures to mitigate consequences. These notes will be useful in completing the final step: risk monitoring. This step mainly involves observing risks and asking the following questions:
- Is risk control effective?
- Were risks correctly classified?
- Have all risks been identified?
Quantitative Risk Analysis Steps
Step 1: identify the purpose, scope, method.
Project managers first need to think about what they want out of the quantitative risk analysis. What kind of insight are they looking for? After identifying the purpose of quantitative risk analysis, project managers can now define the scope and limitations. What data will or will not be included in the quantitative risk analysis? Once this question has been answered, project managers can now select one of the following methods for quantitative risk analysis:
- Failure Mode and Effects Analysis (FMEA)
- Business Impact Analysis (BIA)
- Expected Monetary Value (EMV)
Step 2: Prepare the Data, Tools, and People Needed
Before applying the selected method, project managers should ensure that data is organized and compatible with the method and tools they plan to use. Tools can include digital templates, specialized software such as an employee gps tracking , and other materials that can help in performing quantitative risk analysis. As for the preparation of the people needed, this highly depends on whether or not project managers decide to hire outside experts or involve people from other departments or branches.
Step 3: Apply the Chosen Method to the Data Gathered
Once the data, tools, and people needed are ready, project managers can proceed with performing the quantitative risk analysis. If project managers selected the FMEA or BIA methods, they can use the following digital templates:
- FMEA Template
- BIA Template
For the EMV method, project managers can use the following formula:
Probability in % of Risk Occurring x Cost of Impact in Preferred Currency = EMV
Step 4: Record and Store All Results
After applying the FMEA, BIA, or EMV method, ensure that all results are recorded and stored securely, even if they aren’t the focus of this risk analysis. The reason for keeping these records is that they may be useful later on in the next risk analysis. As quantitative risk analysis takes up a lot of time, effort, and resources, it’s important to not waste information gained from it.
Quantitative risk analysis is also helpful in performing industry-specific functions such as restaurant inspections , pharmaceutical audits , and food safety inspections as it can help identify health code violations before they become a problem.
Achieve operational excellence
Cultivate a culture of excellence with our digital solutions that enhance efficiency, agility, and continuous improvement across all operations.
Leverage Digital and Ready-to-Use Templates
SafetyCulture (formerly iAuditor) templates are easy to use and customize according to the needs of the project. Project managers can simply download one of SafetyCulture’s pre-made templates to get started. Here are some SafetyCulture templates that could help project managers in performing qualitative and quantitative risk analysis:
Quantitative Risk Analysis Template
Use this digital template as a guide in performing quantitative risk analysis. It includes the following steps:
- Identify the purpose, scope, and method
- Prepare the data, tools, and people needed
- Apply the chosen method to the data gathered
- Record and store all results for future risk analysis
Create your own Quantitative Risk Analysis template
Build from scratch or choose from our collection of free, ready-to-download, and customizable templates.
SafetyCulture for Qualitative and Quantitative Risk Analysis
Why safetyculture.
SafetyCulture offers a number of ready-to-use risk analysis templates that can be used in different industries to manage and control risks on-the-go.
Available on Android, iOS, and the web, SafetyCulture is a customizable mobile inspection app mainly used to improve and maintain safety and quality in numerous industries.
- Perform qualitative and quantitative risk analysis on a mobile device
- View qualitative and quantitative risk analysis results in analytics
- Streamline qualitative and quantitative risk analysis processes
SafetyCulture is a digital operations platform project managers use to ensure that their projects stay on track. It has the following features:
Perform risk analysis on a mobile device
SafetyCulture makes it simple and easy for project managers to perform risk analysis on the go or in the field. With the SafetyCulture mobile app , project managers can capture and record risks as soon as they appear, set risk ratings, and collaborate with other members of their team in identifying potential risks.
Create corrective actions to control risks
Project managers can assign corrective actions to anyone in the organization or even to themselves. They can add due dates, priority levels, and images to any corrective action created in SafetyCulture.
Keep risk analysis results all in one place
View risk analysis results in the analytics dashboard, and apply filters to get the insights you need. Store critical data effortlessly with automated recordkeeping.
Reach Project Goals
SafetyCulture helps you manage risks so that they don’t get in the way of your work. Without a good project risk management system and training , projects are vulnerable to unexpected threats and may be delayed as a result. Prepare for anything and everything by identifying and analyzing risks. By performing regular risk analysis, you become more equipped to handle possible obstacles to the project completion.
FAQs about Qualitative and Quantitative Risk Analysis
What does a qualitative risk analysis focus on.
Qualitative risk analysis focuses on assessing and prioritizing risks based on their impact and likelihood, using non-numerical methods. It provides a subjective evaluation based on the perspective of the assessor and the business’s priorities. Qualitative risk analysis also typically doesn’t involve mathematical calculations or quantification.
What are the quantitative risk analysis methods?
Some of the methods used when implementing quantitative risk analysis are Failure Mode and Effects Analysis (FMEA), Business Impact Analysis (BIA), and Expected Monetary Value (EMV). The specific method greatly depends on the needs of the analysis as well as the goal that organizations want to achieve with the results.
When to perform a qualitative and quantitative risk analysis?
Qualitative risk analysis should be performed when there is a change in the perception of risk and when a new risk has been identified. As a general rule, project managers should always perform qualitative risk analysis at the beginning of every project. Additionally, since performing qualitative risk analysis is relatively easy, quick, and low-cost, it can be done at any time during the project or whenever the project manager deems it necessary.
In relation to that, a 5 whys software can help in efficiently performing qualitative risk analysis. Since 5 whys digs into the reason why a certain situation is the way it is, calculating risks and their impact would be easier and more credible.
Quantitative risk analysis should be performed when there is a large amount of data on the risk and its impact and when qualitative risk analysis needs to be validated. Since performing quantitative risk analysis and quantitative risk assessment can be difficult and time-consuming, it is not recommended by most project managers unless the safety of the project relies on precise estimations of risk. In these environments, performing quantitative risk analysis may be required by law or by project stakeholders.
SafetyCulture Content Team
Related articles

- Layer of Protection Analysis
Discover the key aspects of and strategies for LOPA to effectively evaluate and enhance safety systems in high-risk industries.
- Find out more

- Dust Hazard Analysis
Explore the essential components of DHA, its significance, and the strategies for ensuring industrial safety.

- Reputational Risk
Learn more about reputational risk, why it’s important that businesses properly manage it, and how to effectively implement risk mitigation strategies.
Related pages
- Hazard Assessment Software
- Process Hazard Analysis Software
- EHS Risk Assessment Software
- Integrated Risk Management Software
- Operational Risk Management Software
- Reputation Management
- Environmental Aspects and Impacts
- Safety Improvement Plan Template
- Contract Risk Assessment Checklist
- Point of Work Risk Assessment Template
- 7 Best Risk Assessment Templates
- 5×5 Risk Matrix Template
COMMENTS
The research team consisted of academic and clinically based staff. The study adopted a qualitative design, influenced by Grounded theory, to gain in-depth understanding of participants' experiences (Savin-Baden and Major, 2013).
The present study aimed to gather knowledge and insights regarding assessing risk among individuals with disabilities. ... life skills, challenging behavior, and communication. The interviews identified areas of concern that might guide assessment and inform providers about the most individually relevant contexts to consider when supporting ...
This comprehensive article explores strategic risk management in the realm of medical imaging devices, focusing on diagnostic X-ray equipment. While the field is crucial for diagnosing multiple diseases, complete guidelines for risk management and failure analysis covering radiological equipment have been inhibited by rare findings and methodological flaws. This narrative review carefully ...
These factors affect the assessment, treatment, and support of adolescent mothers and help-seeking by mothers. ... strengthening the healthcare system and empowering providers with the knowledge and skills to recognize at-risk mothers and provide timely support is essential. ... Alin S. Qualitative research methods: a comparison between focus ...
Risk Assessment and Analysis Methods: Qualitative and Quantitative. A risk assessment determines the likelihood, consequences and tolerances of possible incidents. "Risk assessment is an inherent part of a broader risk management strategy to introduce control measures to eliminate or reduce any potential risk- related consequences." 1 The ...
Qualitative risk assessment is cheaper and faster, and defines risk in terms of the severity of its impact and the likelihood of its occurrence. Levels of impact and likelihood can be combined into a risk matrix to obtain a measurement of a risk's severity level. Precision ratings of low, medium, and high can be assigned to the risk assessment ...
Abstract. Although the primary "risk assessment" focus of this book addresses quantitative methods, several qualitative methods of risk analysis are widely used for evaluation and decision-making across all industrial, institutional, educational, and commercial organizations. Qualitative analysis methods describe risks in relative terms ...
In John W. Creswell's book, he uses five approaches to qualitative research in both the inquiry and design phases. These are listed as follows: narrative research, phenomenological research, grounded theory research, ethnographic research, and case study research. Quantitative research is the opposite of qualitative research.
A step forward in the qualitative assessment process can be done associating a score to the probability and impact scales: this will allow further possibilities of analysis in particular in terms of: risk factors ranking. risk categories and impact areas relevant "risk" weight on the overall project risk exposure.
Qualitative Risk Assessment Methods. Although the primary "risk assessment" focus of this book addresses quantitative methods, several qualitative methods of risk analysis are widely used for evaluation and decision- making across all industrial, institutional, educational, and commercial organizations. Qualitative analysis methods describe ...
Qualitative assessments reveal data gaps and can be useful in directing resources to productive areas of research. An example of qualitative risk characterization is the hypothetical risk matrix shown in Fig. 5. ... Qualitative risk assessment is not, however, simply a literature review or description of all of the available information about a ...
Traditionally, risk assessments in research have been limited to examining the risks to the research participants. Although doing so is appropriate and important, there is growing recognition that undertaking research can pose risks to researchers as well.
Qualitative risk assessment is a method based on experience, knowledge, and expert questionnaire data. Risks are analyzed and judged based on risk assessors' experience and knowledge, and the ...
Risk assessment is a general term used across many industries to determine the likelihood of loss on a particular asset, investment or loan. The process of assessing risk helps to determine if an ...
Typically, the field of research ethics concerns itself with matters of risk, harm, justice, consequences, benefits, and care (Israel, 2015).Mitigating the risk of psychological (distress) and social (discriminatory judgment) harm is a key consideration in research ethics (Resnik, 2018).Researchers and ethics committees are accustomed to assessing these aspects of proposed research and ...
Qualitative risk assessment is quick to implement due to the lack of statistical/numerical dependence and measurements, and can be performed easily. It is also beneficial if employees are experienced in asset/processes; however, they may also bring biases in determining probability and impact. Qualitative risk analysis is quick but subjective.
There is a general research focus on dynamic risk assessment and management rather than static or traditional risk assessment. ... Another example is security-type applications, where qualitative assessments are often performed on the basis of judgements of actors' intentions and capacities, without reference to a probability scale. ...
Qualitative risk analysis is an essential part of risk management framework and risk assessment process in all organizations. Qualitative risk analysis is a management technique concerned with examining the probability of a risky event and the impact of the risk if it occurs. All risks have both probability and impact that characterizes the risk.
Although the primary "risk assessment" focus of this book addresses quantitative methods, several qualitative methods of risk analysis are widely used for evaluation and decision-making across ...
The qualitative method focuses on detecting procedures and logical reasoning (Patton, 1987), incorporates experience, knowledge, and creativity (Emblemsvåg et al., 2006), and is grounded in ...
Qualitative analysis of risk serves 3 functions: Prioritise risks according to probability & impact. Identify the main areas of risk exposure. Improve understanding of project risks. Projects are exposed to all sorts of risks and it's impractical for project managers to deal with all of them.
Risk Probability and Impact Assessment. This method involves looking into the likelihood of each risk and the ways it may affect separate project objectives, such as those tied to budget, schedule and performance. In this case, negative effects are "threats" and positive effects are "opportunities.". This type of assessment is generally ...
Traditionally, risk assessments in research have been limited to examining the risks to the research participants. Although doing so is appropriate and important, there is growing recognition that undertaking research can pose risks to researchers as well. ... Risk to researchers in qualitative research on sensitive topics: issues and ...
Qualitative Risk Analysis & Other Types of Risk Assessment. Choosing the right risk assessment methodology, whether qualitative, quantitative, or both, is crucial for effectively managing threats. "Research the threat and apply data from sources like public records, social media, dark net—so that you can learn as much as possible.".
Research risk assessment. It's the responsibility of the principal investigators (PI) and researchers to identify reasonably foreseeable risks associated with their research and control the risks so far as is reasonably practicable. All participants and research assistants have the right to expect protection from physical, psychological, social ...
As mentioned earlier, qualitative risk analysis is based on a person's perception or judgment while quantitative risk analysis is based on verified and specific data. Another difference is the values associated with risks. In qualitative risk analysis, this value is the risk rating or scoring. A risk may be rated "Low" or given a score of ...
Abstract. Traditionally, risk assessments in research have been limited to examining the risks to the research participants. Although doing so is appropriate and important, there is growing ...