
Chapter 11. Interviewing
Introduction.
Interviewing people is at the heart of qualitative research. It is not merely a way to collect data but an intrinsically rewarding activity—an interaction between two people that holds the potential for greater understanding and interpersonal development. Unlike many of our daily interactions with others that are fairly shallow and mundane, sitting down with a person for an hour or two and really listening to what they have to say is a profound and deep enterprise, one that can provide not only “data” for you, the interviewer, but also self-understanding and a feeling of being heard for the interviewee. I always approach interviewing with a deep appreciation for the opportunity it gives me to understand how other people experience the world. That said, there is not one kind of interview but many, and some of these are shallower than others. This chapter will provide you with an overview of interview techniques but with a special focus on the in-depth semistructured interview guide approach, which is the approach most widely used in social science research.
An interview can be variously defined as “a conversation with a purpose” ( Lune and Berg 2018 ) and an attempt to understand the world from the point of view of the person being interviewed: “to unfold the meaning of peoples’ experiences, to uncover their lived world prior to scientific explanations” ( Kvale 2007 ). It is a form of active listening in which the interviewer steers the conversation to subjects and topics of interest to their research but also manages to leave enough space for those interviewed to say surprising things. Achieving that balance is a tricky thing, which is why most practitioners believe interviewing is both an art and a science. In my experience as a teacher, there are some students who are “natural” interviewers (often they are introverts), but anyone can learn to conduct interviews, and everyone, even those of us who have been doing this for years, can improve their interviewing skills. This might be a good time to highlight the fact that the interview is a product between interviewer and interviewee and that this product is only as good as the rapport established between the two participants. Active listening is the key to establishing this necessary rapport.
Patton ( 2002 ) makes the argument that we use interviews because there are certain things that are not observable. In particular, “we cannot observe feelings, thoughts, and intentions. We cannot observe behaviors that took place at some previous point in time. We cannot observe situations that preclude the presence of an observer. We cannot observe how people have organized the world and the meanings they attach to what goes on in the world. We have to ask people questions about those things” ( 341 ).
Types of Interviews
There are several distinct types of interviews. Imagine a continuum (figure 11.1). On one side are unstructured conversations—the kind you have with your friends. No one is in control of those conversations, and what you talk about is often random—whatever pops into your head. There is no secret, underlying purpose to your talking—if anything, the purpose is to talk to and engage with each other, and the words you use and the things you talk about are a little beside the point. An unstructured interview is a little like this informal conversation, except that one of the parties to the conversation (you, the researcher) does have an underlying purpose, and that is to understand the other person. You are not friends speaking for no purpose, but it might feel just as unstructured to the “interviewee” in this scenario. That is one side of the continuum. On the other side are fully structured and standardized survey-type questions asked face-to-face. Here it is very clear who is asking the questions and who is answering them. This doesn’t feel like a conversation at all! A lot of people new to interviewing have this ( erroneously !) in mind when they think about interviews as data collection. Somewhere in the middle of these two extreme cases is the “ semistructured” interview , in which the researcher uses an “interview guide” to gently move the conversation to certain topics and issues. This is the primary form of interviewing for qualitative social scientists and will be what I refer to as interviewing for the rest of this chapter, unless otherwise specified.

Informal (unstructured conversations). This is the most “open-ended” approach to interviewing. It is particularly useful in conjunction with observational methods (see chapters 13 and 14). There are no predetermined questions. Each interview will be different. Imagine you are researching the Oregon Country Fair, an annual event in Veneta, Oregon, that includes live music, artisan craft booths, face painting, and a lot of people walking through forest paths. It’s unlikely that you will be able to get a person to sit down with you and talk intensely about a set of questions for an hour and a half. But you might be able to sidle up to several people and engage with them about their experiences at the fair. You might have a general interest in what attracts people to these events, so you could start a conversation by asking strangers why they are here or why they come back every year. That’s it. Then you have a conversation that may lead you anywhere. Maybe one person tells a long story about how their parents brought them here when they were a kid. A second person talks about how this is better than Burning Man. A third person shares their favorite traveling band. And yet another enthuses about the public library in the woods. During your conversations, you also talk about a lot of other things—the weather, the utilikilts for sale, the fact that a favorite food booth has disappeared. It’s all good. You may not be able to record these conversations. Instead, you might jot down notes on the spot and then, when you have the time, write down as much as you can remember about the conversations in long fieldnotes. Later, you will have to sit down with these fieldnotes and try to make sense of all the information (see chapters 18 and 19).
Interview guide ( semistructured interview ). This is the primary type employed by social science qualitative researchers. The researcher creates an “interview guide” in advance, which she uses in every interview. In theory, every person interviewed is asked the same questions. In practice, every person interviewed is asked mostly the same topics but not always the same questions, as the whole point of a “guide” is that it guides the direction of the conversation but does not command it. The guide is typically between five and ten questions or question areas, sometimes with suggested follow-ups or prompts . For example, one question might be “What was it like growing up in Eastern Oregon?” with prompts such as “Did you live in a rural area? What kind of high school did you attend?” to help the conversation develop. These interviews generally take place in a quiet place (not a busy walkway during a festival) and are recorded. The recordings are transcribed, and those transcriptions then become the “data” that is analyzed (see chapters 18 and 19). The conventional length of one of these types of interviews is between one hour and two hours, optimally ninety minutes. Less than one hour doesn’t allow for much development of questions and thoughts, and two hours (or more) is a lot of time to ask someone to sit still and answer questions. If you have a lot of ground to cover, and the person is willing, I highly recommend two separate interview sessions, with the second session being slightly shorter than the first (e.g., ninety minutes the first day, sixty minutes the second). There are lots of good reasons for this, but the most compelling one is that this allows you to listen to the first day’s recording and catch anything interesting you might have missed in the moment and so develop follow-up questions that can probe further. This also allows the person being interviewed to have some time to think about the issues raised in the interview and go a little deeper with their answers.
Standardized questionnaire with open responses ( structured interview ). This is the type of interview a lot of people have in mind when they hear “interview”: a researcher comes to your door with a clipboard and proceeds to ask you a series of questions. These questions are all the same whoever answers the door; they are “standardized.” Both the wording and the exact order are important, as people’s responses may vary depending on how and when a question is asked. These are qualitative only in that the questions allow for “open-ended responses”: people can say whatever they want rather than select from a predetermined menu of responses. For example, a survey I collaborated on included this open-ended response question: “How does class affect one’s career success in sociology?” Some of the answers were simply one word long (e.g., “debt”), and others were long statements with stories and personal anecdotes. It is possible to be surprised by the responses. Although it’s a stretch to call this kind of questioning a conversation, it does allow the person answering the question some degree of freedom in how they answer.
Survey questionnaire with closed responses (not an interview!). Standardized survey questions with specific answer options (e.g., closed responses) are not really interviews at all, and they do not generate qualitative data. For example, if we included five options for the question “How does class affect one’s career success in sociology?”—(1) debt, (2) social networks, (3) alienation, (4) family doesn’t understand, (5) type of grad program—we leave no room for surprises at all. Instead, we would most likely look at patterns around these responses, thinking quantitatively rather than qualitatively (e.g., using regression analysis techniques, we might find that working-class sociologists were twice as likely to bring up alienation). It can sometimes be confusing for new students because the very same survey can include both closed-ended and open-ended questions. The key is to think about how these will be analyzed and to what level surprises are possible. If your plan is to turn all responses into a number and make predictions about correlations and relationships, you are no longer conducting qualitative research. This is true even if you are conducting this survey face-to-face with a real live human. Closed-response questions are not conversations of any kind, purposeful or not.
In summary, the semistructured interview guide approach is the predominant form of interviewing for social science qualitative researchers because it allows a high degree of freedom of responses from those interviewed (thus allowing for novel discoveries) while still maintaining some connection to a research question area or topic of interest. The rest of the chapter assumes the employment of this form.
Creating an Interview Guide
Your interview guide is the instrument used to bridge your research question(s) and what the people you are interviewing want to tell you. Unlike a standardized questionnaire, the questions actually asked do not need to be exactly what you have written down in your guide. The guide is meant to create space for those you are interviewing to talk about the phenomenon of interest, but sometimes you are not even sure what that phenomenon is until you start asking questions. A priority in creating an interview guide is to ensure it offers space. One of the worst mistakes is to create questions that are so specific that the person answering them will not stray. Relatedly, questions that sound “academic” will shut down a lot of respondents. A good interview guide invites respondents to talk about what is important to them, not feel like they are performing or being evaluated by you.
Good interview questions should not sound like your “research question” at all. For example, let’s say your research question is “How do patriarchal assumptions influence men’s understanding of climate change and responses to climate change?” It would be worse than unhelpful to ask a respondent, “How do your assumptions about the role of men affect your understanding of climate change?” You need to unpack this into manageable nuggets that pull your respondent into the area of interest without leading him anywhere. You could start by asking him what he thinks about climate change in general. Or, even better, whether he has any concerns about heatwaves or increased tornadoes or polar icecaps melting. Once he starts talking about that, you can ask follow-up questions that bring in issues around gendered roles, perhaps asking if he is married (to a woman) and whether his wife shares his thoughts and, if not, how they negotiate that difference. The fact is, you won’t really know the right questions to ask until he starts talking.
There are several distinct types of questions that can be used in your interview guide, either as main questions or as follow-up probes. If you remember that the point is to leave space for the respondent, you will craft a much more effective interview guide! You will also want to think about the place of time in both the questions themselves (past, present, future orientations) and the sequencing of the questions.
Researcher Note
Suggestion : As you read the next three sections (types of questions, temporality, question sequence), have in mind a particular research question, and try to draft questions and sequence them in a way that opens space for a discussion that helps you answer your research question.
Type of Questions
Experience and behavior questions ask about what a respondent does regularly (their behavior) or has done (their experience). These are relatively easy questions for people to answer because they appear more “factual” and less subjective. This makes them good opening questions. For the study on climate change above, you might ask, “Have you ever experienced an unusual weather event? What happened?” Or “You said you work outside? What is a typical summer workday like for you? How do you protect yourself from the heat?”
Opinion and values questions , in contrast, ask questions that get inside the minds of those you are interviewing. “Do you think climate change is real? Who or what is responsible for it?” are two such questions. Note that you don’t have to literally ask, “What is your opinion of X?” but you can find a way to ask the specific question relevant to the conversation you are having. These questions are a bit trickier to ask because the answers you get may depend in part on how your respondent perceives you and whether they want to please you or not. We’ve talked a fair amount about being reflective. Here is another place where this comes into play. You need to be aware of the effect your presence might have on the answers you are receiving and adjust accordingly. If you are a woman who is perceived as liberal asking a man who identifies as conservative about climate change, there is a lot of subtext that can be going on in the interview. There is no one right way to resolve this, but you must at least be aware of it.
Feeling questions are questions that ask respondents to draw on their emotional responses. It’s pretty common for academic researchers to forget that we have bodies and emotions, but people’s understandings of the world often operate at this affective level, sometimes unconsciously or barely consciously. It is a good idea to include questions that leave space for respondents to remember, imagine, or relive emotional responses to particular phenomena. “What was it like when you heard your cousin’s house burned down in that wildfire?” doesn’t explicitly use any emotion words, but it allows your respondent to remember what was probably a pretty emotional day. And if they respond emotionally neutral, that is pretty interesting data too. Note that asking someone “How do you feel about X” is not always going to evoke an emotional response, as they might simply turn around and respond with “I think that…” It is better to craft a question that actually pushes the respondent into the affective category. This might be a specific follow-up to an experience and behavior question —for example, “You just told me about your daily routine during the summer heat. Do you worry it is going to get worse?” or “Have you ever been afraid it will be too hot to get your work accomplished?”
Knowledge questions ask respondents what they actually know about something factual. We have to be careful when we ask these types of questions so that respondents do not feel like we are evaluating them (which would shut them down), but, for example, it is helpful to know when you are having a conversation about climate change that your respondent does in fact know that unusual weather events have increased and that these have been attributed to climate change! Asking these questions can set the stage for deeper questions and can ensure that the conversation makes the same kind of sense to both participants. For example, a conversation about political polarization can be put back on track once you realize that the respondent doesn’t really have a clear understanding that there are two parties in the US. Instead of asking a series of questions about Republicans and Democrats, you might shift your questions to talk more generally about political disagreements (e.g., “people against abortion”). And sometimes what you do want to know is the level of knowledge about a particular program or event (e.g., “Are you aware you can discharge your student loans through the Public Service Loan Forgiveness program?”).
Sensory questions call on all senses of the respondent to capture deeper responses. These are particularly helpful in sparking memory. “Think back to your childhood in Eastern Oregon. Describe the smells, the sounds…” Or you could use these questions to help a person access the full experience of a setting they customarily inhabit: “When you walk through the doors to your office building, what do you see? Hear? Smell?” As with feeling questions , these questions often supplement experience and behavior questions . They are another way of allowing your respondent to report fully and deeply rather than remain on the surface.
Creative questions employ illustrative examples, suggested scenarios, or simulations to get respondents to think more deeply about an issue, topic, or experience. There are many options here. In The Trouble with Passion , Erin Cech ( 2021 ) provides a scenario in which “Joe” is trying to decide whether to stay at his decent but boring computer job or follow his passion by opening a restaurant. She asks respondents, “What should Joe do?” Their answers illuminate the attraction of “passion” in job selection. In my own work, I have used a news story about an upwardly mobile young man who no longer has time to see his mother and sisters to probe respondents’ feelings about the costs of social mobility. Jessi Streib and Betsy Leondar-Wright have used single-page cartoon “scenes” to elicit evaluations of potential racial discrimination, sexual harassment, and classism. Barbara Sutton ( 2010 ) has employed lists of words (“strong,” “mother,” “victim”) on notecards she fans out and asks her female respondents to select and discuss.
Background/Demographic Questions
You most definitely will want to know more about the person you are interviewing in terms of conventional demographic information, such as age, race, gender identity, occupation, and educational attainment. These are not questions that normally open up inquiry. [1] For this reason, my practice has been to include a separate “demographic questionnaire” sheet that I ask each respondent to fill out at the conclusion of the interview. Only include those aspects that are relevant to your study. For example, if you are not exploring religion or religious affiliation, do not include questions about a person’s religion on the demographic sheet. See the example provided at the end of this chapter.
Temporality
Any type of question can have a past, present, or future orientation. For example, if you are asking a behavior question about workplace routine, you might ask the respondent to talk about past work, present work, and ideal (future) work. Similarly, if you want to understand how people cope with natural disasters, you might ask your respondent how they felt then during the wildfire and now in retrospect and whether and to what extent they have concerns for future wildfire disasters. It’s a relatively simple suggestion—don’t forget to ask about past, present, and future—but it can have a big impact on the quality of the responses you receive.
Question Sequence
Having a list of good questions or good question areas is not enough to make a good interview guide. You will want to pay attention to the order in which you ask your questions. Even though any one respondent can derail this order (perhaps by jumping to answer a question you haven’t yet asked), a good advance plan is always helpful. When thinking about sequence, remember that your goal is to get your respondent to open up to you and to say things that might surprise you. To establish rapport, it is best to start with nonthreatening questions. Asking about the present is often the safest place to begin, followed by the past (they have to know you a little bit to get there), and lastly, the future (talking about hopes and fears requires the most rapport). To allow for surprises, it is best to move from very general questions to more particular questions only later in the interview. This ensures that respondents have the freedom to bring up the topics that are relevant to them rather than feel like they are constrained to answer you narrowly. For example, refrain from asking about particular emotions until these have come up previously—don’t lead with them. Often, your more particular questions will emerge only during the course of the interview, tailored to what is emerging in conversation.
Once you have a set of questions, read through them aloud and imagine you are being asked the same questions. Does the set of questions have a natural flow? Would you be willing to answer the very first question to a total stranger? Does your sequence establish facts and experiences before moving on to opinions and values? Did you include prefatory statements, where necessary; transitions; and other announcements? These can be as simple as “Hey, we talked a lot about your experiences as a barista while in college.… Now I am turning to something completely different: how you managed friendships in college.” That is an abrupt transition, but it has been softened by your acknowledgment of that.
Probes and Flexibility
Once you have the interview guide, you will also want to leave room for probes and follow-up questions. As in the sample probe included here, you can write out the obvious probes and follow-up questions in advance. You might not need them, as your respondent might anticipate them and include full responses to the original question. Or you might need to tailor them to how your respondent answered the question. Some common probes and follow-up questions include asking for more details (When did that happen? Who else was there?), asking for elaboration (Could you say more about that?), asking for clarification (Does that mean what I think it means or something else? I understand what you mean, but someone else reading the transcript might not), and asking for contrast or comparison (How did this experience compare with last year’s event?). “Probing is a skill that comes from knowing what to look for in the interview, listening carefully to what is being said and what is not said, and being sensitive to the feedback needs of the person being interviewed” ( Patton 2002:374 ). It takes work! And energy. I and many other interviewers I know report feeling emotionally and even physically drained after conducting an interview. You are tasked with active listening and rearranging your interview guide as needed on the fly. If you only ask the questions written down in your interview guide with no deviations, you are doing it wrong. [2]
The Final Question
Every interview guide should include a very open-ended final question that allows for the respondent to say whatever it is they have been dying to tell you but you’ve forgotten to ask. About half the time they are tired too and will tell you they have nothing else to say. But incredibly, some of the most honest and complete responses take place here, at the end of a long interview. You have to realize that the person being interviewed is often discovering things about themselves as they talk to you and that this process of discovery can lead to new insights for them. Making space at the end is therefore crucial. Be sure you convey that you actually do want them to tell you more, that the offer of “anything else?” is not read as an empty convention where the polite response is no. Here is where you can pull from that active listening and tailor the final question to the particular person. For example, “I’ve asked you a lot of questions about what it was like to live through that wildfire. I’m wondering if there is anything I’ve forgotten to ask, especially because I haven’t had that experience myself” is a much more inviting final question than “Great. Anything you want to add?” It’s also helpful to convey to the person that you have the time to listen to their full answer, even if the allotted time is at the end. After all, there are no more questions to ask, so the respondent knows exactly how much time is left. Do them the courtesy of listening to them!
Conducting the Interview
Once you have your interview guide, you are on your way to conducting your first interview. I always practice my interview guide with a friend or family member. I do this even when the questions don’t make perfect sense for them, as it still helps me realize which questions make no sense, are poorly worded (too academic), or don’t follow sequentially. I also practice the routine I will use for interviewing, which goes something like this:
- Introduce myself and reintroduce the study
- Provide consent form and ask them to sign and retain/return copy
- Ask if they have any questions about the study before we begin
- Ask if I can begin recording
- Ask questions (from interview guide)
- Turn off the recording device
- Ask if they are willing to fill out my demographic questionnaire
- Collect questionnaire and, without looking at the answers, place in same folder as signed consent form
- Thank them and depart
A note on remote interviewing: Interviews have traditionally been conducted face-to-face in a private or quiet public setting. You don’t want a lot of background noise, as this will make transcriptions difficult. During the recent global pandemic, many interviewers, myself included, learned the benefits of interviewing remotely. Although face-to-face is still preferable for many reasons, Zoom interviewing is not a bad alternative, and it does allow more interviews across great distances. Zoom also includes automatic transcription, which significantly cuts down on the time it normally takes to convert our conversations into “data” to be analyzed. These automatic transcriptions are not perfect, however, and you will still need to listen to the recording and clarify and clean up the transcription. Nor do automatic transcriptions include notations of body language or change of tone, which you may want to include. When interviewing remotely, you will want to collect the consent form before you meet: ask them to read, sign, and return it as an email attachment. I think it is better to ask for the demographic questionnaire after the interview, but because some respondents may never return it then, it is probably best to ask for this at the same time as the consent form, in advance of the interview.
What should you bring to the interview? I would recommend bringing two copies of the consent form (one for you and one for the respondent), a demographic questionnaire, a manila folder in which to place the signed consent form and filled-out demographic questionnaire, a printed copy of your interview guide (I print with three-inch right margins so I can jot down notes on the page next to relevant questions), a pen, a recording device, and water.
After the interview, you will want to secure the signed consent form in a locked filing cabinet (if in print) or a password-protected folder on your computer. Using Excel or a similar program that allows tables/spreadsheets, create an identifying number for your interview that links to the consent form without using the name of your respondent. For example, let’s say that I conduct interviews with US politicians, and the first person I meet with is George W. Bush. I will assign the transcription the number “INT#001” and add it to the signed consent form. [3] The signed consent form goes into a locked filing cabinet, and I never use the name “George W. Bush” again. I take the information from the demographic sheet, open my Excel spreadsheet, and add the relevant information in separate columns for the row INT#001: White, male, Republican. When I interview Bill Clinton as my second interview, I include a second row: INT#002: White, male, Democrat. And so on. The only link to the actual name of the respondent and this information is the fact that the consent form (unavailable to anyone but me) has stamped on it the interview number.
Many students get very nervous before their first interview. Actually, many of us are always nervous before the interview! But do not worry—this is normal, and it does pass. Chances are, you will be pleasantly surprised at how comfortable it begins to feel. These “purposeful conversations” are often a delight for both participants. This is not to say that sometimes things go wrong. I often have my students practice several “bad scenarios” (e.g., a respondent that you cannot get to open up; a respondent who is too talkative and dominates the conversation, steering it away from the topics you are interested in; emotions that completely take over; or shocking disclosures you are ill-prepared to handle), but most of the time, things go quite well. Be prepared for the unexpected, but know that the reason interviews are so popular as a technique of data collection is that they are usually richly rewarding for both participants.
One thing that I stress to my methods students and remind myself about is that interviews are still conversations between people. If there’s something you might feel uncomfortable asking someone about in a “normal” conversation, you will likely also feel a bit of discomfort asking it in an interview. Maybe more importantly, your respondent may feel uncomfortable. Social research—especially about inequality—can be uncomfortable. And it’s easy to slip into an abstract, intellectualized, or removed perspective as an interviewer. This is one reason trying out interview questions is important. Another is that sometimes the question sounds good in your head but doesn’t work as well out loud in practice. I learned this the hard way when a respondent asked me how I would answer the question I had just posed, and I realized that not only did I not really know how I would answer it, but I also wasn’t quite as sure I knew what I was asking as I had thought.
—Elizabeth M. Lee, Associate Professor of Sociology at Saint Joseph’s University, author of Class and Campus Life , and co-author of Geographies of Campus Inequality
How Many Interviews?
Your research design has included a targeted number of interviews and a recruitment plan (see chapter 5). Follow your plan, but remember that “ saturation ” is your goal. You interview as many people as you can until you reach a point at which you are no longer surprised by what they tell you. This means not that no one after your first twenty interviews will have surprising, interesting stories to tell you but rather that the picture you are forming about the phenomenon of interest to you from a research perspective has come into focus, and none of the interviews are substantially refocusing that picture. That is when you should stop collecting interviews. Note that to know when you have reached this, you will need to read your transcripts as you go. More about this in chapters 18 and 19.
Your Final Product: The Ideal Interview Transcript
A good interview transcript will demonstrate a subtly controlled conversation by the skillful interviewer. In general, you want to see replies that are about one paragraph long, not short sentences and not running on for several pages. Although it is sometimes necessary to follow respondents down tangents, it is also often necessary to pull them back to the questions that form the basis of your research study. This is not really a free conversation, although it may feel like that to the person you are interviewing.
Final Tips from an Interview Master
Annette Lareau is arguably one of the masters of the trade. In Listening to People , she provides several guidelines for good interviews and then offers a detailed example of an interview gone wrong and how it could be addressed (please see the “Further Readings” at the end of this chapter). Here is an abbreviated version of her set of guidelines: (1) interview respondents who are experts on the subjects of most interest to you (as a corollary, don’t ask people about things they don’t know); (2) listen carefully and talk as little as possible; (3) keep in mind what you want to know and why you want to know it; (4) be a proactive interviewer (subtly guide the conversation); (5) assure respondents that there aren’t any right or wrong answers; (6) use the respondent’s own words to probe further (this both allows you to accurately identify what you heard and pushes the respondent to explain further); (7) reuse effective probes (don’t reinvent the wheel as you go—if repeating the words back works, do it again and again); (8) focus on learning the subjective meanings that events or experiences have for a respondent; (9) don’t be afraid to ask a question that draws on your own knowledge (unlike trial lawyers who are trained never to ask a question for which they don’t already know the answer, sometimes it’s worth it to ask risky questions based on your hypotheses or just plain hunches); (10) keep thinking while you are listening (so difficult…and important); (11) return to a theme raised by a respondent if you want further information; (12) be mindful of power inequalities (and never ever coerce a respondent to continue the interview if they want out); (13) take control with overly talkative respondents; (14) expect overly succinct responses, and develop strategies for probing further; (15) balance digging deep and moving on; (16) develop a plan to deflect questions (e.g., let them know you are happy to answer any questions at the end of the interview, but you don’t want to take time away from them now); and at the end, (17) check to see whether you have asked all your questions. You don’t always have to ask everyone the same set of questions, but if there is a big area you have forgotten to cover, now is the time to recover ( Lareau 2021:93–103 ).
Sample: Demographic Questionnaire
ASA Taskforce on First-Generation and Working-Class Persons in Sociology – Class Effects on Career Success
Supplementary Demographic Questionnaire
Thank you for your participation in this interview project. We would like to collect a few pieces of key demographic information from you to supplement our analyses. Your answers to these questions will be kept confidential and stored by ID number. All of your responses here are entirely voluntary!
What best captures your race/ethnicity? (please check any/all that apply)
- White (Non Hispanic/Latina/o/x)
- Black or African American
- Hispanic, Latino/a/x of Spanish
- Asian or Asian American
- American Indian or Alaska Native
- Middle Eastern or North African
- Native Hawaiian or Pacific Islander
- Other : (Please write in: ________________)
What is your current position?
- Grad Student
- Full Professor
Please check any and all of the following that apply to you:
- I identify as a working-class academic
- I was the first in my family to graduate from college
- I grew up poor
What best reflects your gender?
- Transgender female/Transgender woman
- Transgender male/Transgender man
- Gender queer/ Gender nonconforming
Anything else you would like us to know about you?
Example: Interview Guide
In this example, follow-up prompts are italicized. Note the sequence of questions. That second question often elicits an entire life history , answering several later questions in advance.
Introduction Script/Question
Thank you for participating in our survey of ASA members who identify as first-generation or working-class. As you may have heard, ASA has sponsored a taskforce on first-generation and working-class persons in sociology and we are interested in hearing from those who so identify. Your participation in this interview will help advance our knowledge in this area.
- The first thing we would like to as you is why you have volunteered to be part of this study? What does it mean to you be first-gen or working class? Why were you willing to be interviewed?
- How did you decide to become a sociologist?
- Can you tell me a little bit about where you grew up? ( prompts: what did your parent(s) do for a living? What kind of high school did you attend?)
- Has this identity been salient to your experience? (how? How much?)
- How welcoming was your grad program? Your first academic employer?
- Why did you decide to pursue sociology at the graduate level?
- Did you experience culture shock in college? In graduate school?
- Has your FGWC status shaped how you’ve thought about where you went to school? debt? etc?
- Were you mentored? How did this work (not work)? How might it?
- What did you consider when deciding where to go to grad school? Where to apply for your first position?
- What, to you, is a mark of career success? Have you achieved that success? What has helped or hindered your pursuit of success?
- Do you think sociology, as a field, cares about prestige?
- Let’s talk a little bit about intersectionality. How does being first-gen/working class work alongside other identities that are important to you?
- What do your friends and family think about your career? Have you had any difficulty relating to family members or past friends since becoming highly educated?
- Do you have any debt from college/grad school? Are you concerned about this? Could you explain more about how you paid for college/grad school? (here, include assistance from family, fellowships, scholarships, etc.)
- (You’ve mentioned issues or obstacles you had because of your background.) What could have helped? Or, who or what did? Can you think of fortuitous moments in your career?
- Do you have any regrets about the path you took?
- Is there anything else you would like to add? Anything that the Taskforce should take note of, that we did not ask you about here?
Further Readings
Britten, Nicky. 1995. “Qualitative Interviews in Medical Research.” BMJ: British Medical Journal 31(6999):251–253. A good basic overview of interviewing particularly useful for students of public health and medical research generally.
Corbin, Juliet, and Janice M. Morse. 2003. “The Unstructured Interactive Interview: Issues of Reciprocity and Risks When Dealing with Sensitive Topics.” Qualitative Inquiry 9(3):335–354. Weighs the potential benefits and harms of conducting interviews on topics that may cause emotional distress. Argues that the researcher’s skills and code of ethics should ensure that the interviewing process provides more of a benefit to both participant and researcher than a harm to the former.
Gerson, Kathleen, and Sarah Damaske. 2020. The Science and Art of Interviewing . New York: Oxford University Press. A useful guidebook/textbook for both undergraduates and graduate students, written by sociologists.
Kvale, Steiner. 2007. Doing Interviews . London: SAGE. An easy-to-follow guide to conducting and analyzing interviews by psychologists.
Lamont, Michèle, and Ann Swidler. 2014. “Methodological Pluralism and the Possibilities and Limits of Interviewing.” Qualitative Sociology 37(2):153–171. Written as a response to various debates surrounding the relative value of interview-based studies and ethnographic studies defending the particular strengths of interviewing. This is a must-read article for anyone seriously engaging in qualitative research!
Pugh, Allison J. 2013. “What Good Are Interviews for Thinking about Culture? Demystifying Interpretive Analysis.” American Journal of Cultural Sociology 1(1):42–68. Another defense of interviewing written against those who champion ethnographic methods as superior, particularly in the area of studying culture. A classic.
Rapley, Timothy John. 2001. “The ‘Artfulness’ of Open-Ended Interviewing: Some considerations in analyzing interviews.” Qualitative Research 1(3):303–323. Argues for the importance of “local context” of data production (the relationship built between interviewer and interviewee, for example) in properly analyzing interview data.
Weiss, Robert S. 1995. Learning from Strangers: The Art and Method of Qualitative Interview Studies . New York: Simon and Schuster. A classic and well-regarded textbook on interviewing. Because Weiss has extensive experience conducting surveys, he contrasts the qualitative interview with the survey questionnaire well; particularly useful for those trained in the latter.
- I say “normally” because how people understand their various identities can itself be an expansive topic of inquiry. Here, I am merely talking about collecting otherwise unexamined demographic data, similar to how we ask people to check boxes on surveys. ↵
- Again, this applies to “semistructured in-depth interviewing.” When conducting standardized questionnaires, you will want to ask each question exactly as written, without deviations! ↵
- I always include “INT” in the number because I sometimes have other kinds of data with their own numbering: FG#001 would mean the first focus group, for example. I also always include three-digit spaces, as this allows for up to 999 interviews (or, more realistically, allows for me to interview up to one hundred persons without having to reset my numbering system). ↵
A method of data collection in which the researcher asks the participant questions; the answers to these questions are often recorded and transcribed verbatim. There are many different kinds of interviews - see also semistructured interview , structured interview , and unstructured interview .
A document listing key questions and question areas for use during an interview. It is used most often for semi-structured interviews. A good interview guide may have no more than ten primary questions for two hours of interviewing, but these ten questions will be supplemented by probes and relevant follow-ups throughout the interview. Most IRBs require the inclusion of the interview guide in applications for review. See also interview and semi-structured interview .
A data-collection method that relies on casual, conversational, and informal interviewing. Despite its apparent conversational nature, the researcher usually has a set of particular questions or question areas in mind but allows the interview to unfold spontaneously. This is a common data-collection technique among ethnographers. Compare to the semi-structured or in-depth interview .
A form of interview that follows a standard guide of questions asked, although the order of the questions may change to match the particular needs of each individual interview subject, and probing “follow-up” questions are often added during the course of the interview. The semi-structured interview is the primary form of interviewing used by qualitative researchers in the social sciences. It is sometimes referred to as an “in-depth” interview. See also interview and interview guide .
The cluster of data-collection tools and techniques that involve observing interactions between people, the behaviors, and practices of individuals (sometimes in contrast to what they say about how they act and behave), and cultures in context. Observational methods are the key tools employed by ethnographers and Grounded Theory .
Follow-up questions used in a semi-structured interview to elicit further elaboration. Suggested prompts can be included in the interview guide to be used/deployed depending on how the initial question was answered or if the topic of the prompt does not emerge spontaneously.
A form of interview that follows a strict set of questions, asked in a particular order, for all interview subjects. The questions are also the kind that elicits short answers, and the data is more “informative” than probing. This is often used in mixed-methods studies, accompanying a survey instrument. Because there is no room for nuance or the exploration of meaning in structured interviews, qualitative researchers tend to employ semi-structured interviews instead. See also interview.
The point at which you can conclude data collection because every person you are interviewing, the interaction you are observing, or content you are analyzing merely confirms what you have already noted. Achieving saturation is often used as the justification for the final sample size.
An interview variant in which a person’s life story is elicited in a narrative form. Turning points and key themes are established by the researcher and used as data points for further analysis.
Introduction to Qualitative Research Methods Copyright © 2023 by Allison Hurst is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License , except where otherwise noted.
- University Libraries
- Research Guides
- Topic Guides
- Research Methods Guide
- Interview Research
Research Methods Guide: Interview Research
- Introduction
- Research Design & Method
- Survey Research
- Data Analysis
- Resources & Consultation
Tutorial Videos: Interview Method
Interview as a Method for Qualitative Research

Goals of Interview Research
- Preferences
- They help you explain, better understand, and explore research subjects' opinions, behavior, experiences, phenomenon, etc.
- Interview questions are usually open-ended questions so that in-depth information will be collected.
Mode of Data Collection
There are several types of interviews, including:
- Face-to-Face
- Online (e.g. Skype, Googlehangout, etc)
FAQ: Conducting Interview Research
What are the important steps involved in interviews?
- Think about who you will interview
- Think about what kind of information you want to obtain from interviews
- Think about why you want to pursue in-depth information around your research topic
- Introduce yourself and explain the aim of the interview
- Devise your questions so interviewees can help answer your research question
- Have a sequence to your questions / topics by grouping them in themes
- Make sure you can easily move back and forth between questions / topics
- Make sure your questions are clear and easy to understand
- Do not ask leading questions
- Do you want to bring a second interviewer with you?
- Do you want to bring a notetaker?
- Do you want to record interviews? If so, do you have time to transcribe interview recordings?
- Where will you interview people? Where is the setting with the least distraction?
- How long will each interview take?
- Do you need to address terms of confidentiality?
Do I have to choose either a survey or interviewing method?
No. In fact, many researchers use a mixed method - interviews can be useful as follow-up to certain respondents to surveys, e.g., to further investigate their responses.
Is training an interviewer important?
Yes, since the interviewer can control the quality of the result, training the interviewer becomes crucial. If more than one interviewers are involved in your study, it is important to have every interviewer understand the interviewing procedure and rehearse the interviewing process before beginning the formal study.
- << Previous: Survey Research
- Next: Data Analysis >>
- Last Updated: Aug 21, 2023 10:42 AM
How to conduct qualitative interviews (tips and best practices)
Last updated
18 May 2023
Reviewed by
Miroslav Damyanov
However, conducting qualitative interviews can be challenging, even for seasoned researchers. Poorly conducted interviews can lead to inaccurate or incomplete data, significantly compromising the validity and reliability of your research findings.
When planning to conduct qualitative interviews, you must adequately prepare yourself to get the most out of your data. Fortunately, there are specific tips and best practices that can help you conduct qualitative interviews effectively.
- What is a qualitative interview?
A qualitative interview is a research technique used to gather in-depth information about people's experiences, attitudes, beliefs, and perceptions. Unlike a structured questionnaire or survey, a qualitative interview is a flexible, conversational approach that allows the interviewer to delve into the interviewee's responses and explore their insights and experiences.
In a qualitative interview, the researcher typically develops a set of open-ended questions that provide a framework for the conversation. However, the interviewer can also adapt to the interviewee's responses and ask follow-up questions to understand their experiences and views better.
- How to conduct interviews in qualitative research
Conducting interviews involves a well-planned and deliberate process to collect accurate and valid data.
Here’s a step-by-step guide on how to conduct interviews in qualitative research, broken down into three stages:
1. Before the interview
The first step in conducting a qualitative interview is determining your research question . This will help you identify the type of participants you need to recruit . Once you have your research question, you can start recruiting participants by identifying potential candidates and contacting them to gauge their interest in participating in the study.
After that, it's time to develop your interview questions. These should be open-ended questions that will elicit detailed responses from participants. You'll also need to get consent from the participants, ideally in writing, to ensure that they understand the purpose of the study and their rights as participants. Finally, choose a comfortable and private location to conduct the interview and prepare the interview guide.
2. During the interview
Start by introducing yourself and explaining the purpose of the study. Establish a rapport by putting the participants at ease and making them feel comfortable. Use the interview guide to ask the questions, but be flexible and ask follow-up questions to gain more insight into the participants' responses.
Take notes during the interview, and ask permission to record the interview for transcription purposes. Be mindful of the time, and cover all the questions in the interview guide.
3. After the interview
Once the interview is over, transcribe the interview if you recorded it. If you took notes, review and organize them to make sure you capture all the important information. Then, analyze the data you collected by identifying common themes and patterns. Use the findings to answer your research question.
Finally, debrief with the participants to thank them for their time, provide feedback on the study, and answer any questions they may have.
Free AI content analysis generator
Make sense of your research by automatically summarizing key takeaways through our free content analysis tool.

- What kinds of questions should you ask in a qualitative interview?
Qualitative interviews involve asking questions that encourage participants to share their experiences, opinions, and perspectives on a particular topic. These questions are designed to elicit detailed and nuanced responses rather than simple yes or no answers.
Effective questions in a qualitative interview are generally open-ended and non-leading. They avoid presuppositions or assumptions about the participant's experience and allow them to share their views in their own words.
In customer research , you might ask questions such as:
What motivated you to choose our product/service over our competitors?
How did you first learn about our product/service?
Can you walk me through your experience with our product/service?
What improvements or changes would you suggest for our product/service?
Have you recommended our product/service to others, and if so, why?
The key is to ask questions relevant to the research topic and allow participants to share their experiences meaningfully and informally.
- How to determine the right qualitative interview participants
Choosing the right participants for a qualitative interview is a crucial step in ensuring the success and validity of the research . You need to consider several factors to determine the right participants for a qualitative interview. These may include:
Relevant experiences : Participants should have experiences related to the research topic that can provide valuable insights.
Diversity : Aim to include diverse participants to ensure the study's findings are representative and inclusive.
Access : Identify participants who are accessible and willing to participate in the study.
Informed consent : Participants should be fully informed about the study's purpose, methods, and potential risks and benefits and be allowed to provide informed consent.
You can use various recruitment methods, such as posting ads in relevant forums, contacting community organizations or social media groups, or using purposive sampling to identify participants who meet specific criteria.
- How to make qualitative interview subjects comfortable
Making participants comfortable during a qualitative interview is essential to obtain rich, detailed data. Participants are more likely to share their experiences openly when they feel at ease and not judged.
Here are some ways to make interview subjects comfortable:
Explain the purpose of the study
Start the interview by explaining the research topic and its importance. The goal is to give participants a sense of what to expect.
Create a comfortable environment
Conduct the interview in a quiet, private space where the participant feels comfortable. Turn off any unnecessary electronics that can create distractions. Ensure your equipment works well ahead of time. Arrive at the interview on time. If you conduct a remote interview, turn on your camera and mute all notetakers and observers.
Build rapport
Greet the participant warmly and introduce yourself. Show interest in their responses and thank them for their time.
Use open-ended questions
Ask questions that encourage participants to elaborate on their thoughts and experiences.
Listen attentively
Resist the urge to multitask . Pay attention to the participant's responses, nod your head, or make supportive comments to show you’re interested in their answers. Avoid interrupting them.
Avoid judgment
Show respect and don't judge the participant's views or experiences. Allow the participant to speak freely without feeling judged or ridiculed.
Offer breaks
If needed, offer breaks during the interview, especially if the topic is sensitive or emotional.
Creating a comfortable environment and establishing rapport with the participant fosters an atmosphere of trust and encourages open communication. This helps participants feel at ease and willing to share their experiences.
- How to analyze a qualitative interview
Analyzing a qualitative interview involves a systematic process of examining the data collected to identify patterns, themes, and meanings that emerge from the responses.
Here are some steps on how to analyze a qualitative interview:
1. Transcription
The first step is transcribing the interview into text format to have a written record of the conversation. This step is essential to ensure that you can refer back to the interview data and identify the important aspects of the interview.
2. Data reduction
Once you’ve transcribed the interview, read through it to identify key themes, patterns, and phrases emerging from the data. This process involves reducing the data into more manageable pieces you can easily analyze.
The next step is to code the data by labeling sections of the text with descriptive words or phrases that reflect the data's content. Coding helps identify key themes and patterns from the interview data.
4. Categorization
After coding, you should group the codes into categories based on their similarities. This process helps to identify overarching themes or sub-themes that emerge from the data.
5. Interpretation
You should then interpret the themes and sub-themes by identifying relationships, contradictions, and meanings that emerge from the data. Interpretation involves analyzing the themes in the context of the research question .
6. Comparison
The next step is comparing the data across participants or groups to identify similarities and differences. This step helps to ensure that the findings aren’t just specific to one participant but can be generalized to the wider population.
7. Triangulation
To ensure the findings are valid and reliable, you should use triangulation by comparing the findings with other sources, such as observations or interview data.
8. Synthesis
The final step is synthesizing the findings by summarizing the key themes and presenting them clearly and concisely. This step involves writing a report that presents the findings in a way that is easy to understand, using quotes and examples from the interview data to illustrate the themes.
- Tips for transcribing a qualitative interview
Transcribing a qualitative interview is a crucial step in the research process. It involves converting the audio or video recording of the interview into written text.
Here are some tips for transcribing a qualitative interview:
Use transcription software
Transcription software can save time and increase accuracy by automatically transcribing audio or video recordings.
Listen carefully
When manually transcribing, listen carefully to the recording to ensure clarity. Pause and rewind the recording as necessary.
Use appropriate formatting
Use a consistent format for transcribing, such as marking pauses, overlaps, and interruptions. Indicate non-verbal cues such as laughter, sighs, or changes in tone.
Edit for clarity
Edit the transcription to ensure clarity and readability. Use standard grammar and punctuation, correct misspellings, and remove filler words like "um" and "ah."
Proofread and edit
Verify the accuracy of the transcription by listening to the recording again and reviewing the notes taken during the interview.
Use timestamps
Add timestamps to the transcription to reference specific interview sections.
Transcribing a qualitative interview can be time-consuming, but it’s essential to ensure the accuracy of the data collected. Following these tips can produce high-quality transcriptions useful for analysis and reporting.
- Why are interview techniques in qualitative research effective?
Unlike quantitative research methods, which rely on numerical data, qualitative research seeks to understand the richness and complexity of human experiences and perspectives.
Interview techniques involve asking open-ended questions that allow participants to express their views and share their stories in their own words. This approach can help researchers to uncover unexpected or surprising insights that may not have been discovered through other research methods.
Interview techniques also allow researchers to establish rapport with participants, creating a comfortable and safe space for them to share their experiences. This can lead to a deeper level of trust and candor, leading to more honest and authentic responses.
- What are the weaknesses of qualitative interviews?
Qualitative interviews are an excellent research approach when used properly, but they have their drawbacks.
The weaknesses of qualitative interviews include the following:
Subjectivity and personal biases
Qualitative interviews rely on the researcher's interpretation of the interviewee's responses. The researcher's biases or preconceptions can affect how the questions are framed and how the responses are interpreted, which can influence results.
Small sample size
The sample size in qualitative interviews is often small, which can limit the generalizability of the results to the larger population.
Data quality
The quality of data collected during interviews can be affected by various factors, such as the interviewee's mood, the setting of the interview, and the interviewer's skills and experience.
Socially desirable responses
Interviewees may provide responses that they believe are socially acceptable rather than truthful or genuine.
Conducting qualitative interviews can be expensive, especially if the researcher must travel to different locations to conduct the interviews.
Time-consuming
The data analysis process can be time-consuming and labor-intensive, as researchers need to transcribe and analyze the data manually.
Despite these weaknesses, qualitative interviews remain a valuable research tool . You can take steps to mitigate the impact of these weaknesses by incorporating the perspectives of other researchers or participants in the analysis process, using multiple data sources , and critically analyzing your biases and assumptions.
Mastering the art of qualitative interviews is an essential skill for businesses looking to gain deep insights into their customers' needs , preferences, and behaviors. By following the tips and best practices outlined in this article, you can conduct interviews that provide you with rich data that you can use to make informed decisions about your products, services, and marketing strategies.
Remember that effective communication, active listening, and proper analysis are critical components of successful qualitative interviews. By incorporating these practices into your customer research, you can gain a competitive edge and build stronger customer relationships.
Should you be using a customer insights hub?
Do you want to discover previous research faster?
Do you share your research findings with others?
Do you analyze research data?
Start for free today, add your research, and get to key insights faster
Editor’s picks
Last updated: 18 April 2023
Last updated: 27 February 2023
Last updated: 22 August 2024
Last updated: 5 February 2023
Last updated: 16 August 2024
Last updated: 9 March 2023
Last updated: 30 April 2024
Last updated: 12 December 2023
Last updated: 11 March 2024
Last updated: 4 July 2024
Last updated: 6 March 2024
Last updated: 5 March 2024
Last updated: 13 May 2024
Latest articles
Related topics, .css-je19u9{-webkit-align-items:flex-end;-webkit-box-align:flex-end;-ms-flex-align:flex-end;align-items:flex-end;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-flex-direction:row;-ms-flex-direction:row;flex-direction:row;-webkit-box-flex-wrap:wrap;-webkit-flex-wrap:wrap;-ms-flex-wrap:wrap;flex-wrap:wrap;-webkit-box-pack:center;-ms-flex-pack:center;-webkit-justify-content:center;justify-content:center;row-gap:0;text-align:center;max-width:671px;}@media (max-width: 1079px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}}@media (max-width: 799px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}} decide what to .css-1kiodld{max-height:56px;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;}@media (max-width: 1079px){.css-1kiodld{display:none;}} build next, decide what to build next, log in or sign up.
Get started for free
Using an interview in a research paper
Consultant contributor: Viviane Ugalde
Using an interview can be an effective primary source for some papers and research projects. Finding an expert in the field or some other person who has knowledge of your topic can allow for you to gather unique information not available elsewhere.
There are four steps to using an interview as a source for your research.
- Know where and how to start.
- Know how to write a good question.
- Know how to conduct an interview.
- Know how to incorporate the interview into your document or project.
Step one: Where to start
First, you should determine your goals and ask yourself these questions:
- Who are the local experts on topic?
- How can I contact these people?
- Does anyone know them to help me setup the interviews?
- Are their phone numbers in the phone book or can I find them on the Internet?
Once you answer these questions and pick your interviewee, get their basic information such as their name, title, and other general details. If you reach out and your interview does not participate, don’t be discouraged. Keep looking for other interview contacts.
Step two: How to write a good question
When you have confirmed an interview, it is not time to come up with questions.
- Learning as much as you can about the person before the interview can help you create questions specific to your interview subject.
- Doing research about your interviewee’s past experience in your topic, or any texts that they have written would be great background research.
When you start to think of questions, write down more questions than you think you’ll need, and prioritize them as you go. Any good questions will answer the 5W and H questions. Asking Who, What, When, Where, Why, and How questions that you need answered for your paper, will help you form a question to ask your interviewee.
When writing a good question, try thinking of something that will help your argument.
- Is your interviewee an advocate for you position?
- Are they in any programs that are related to your research?
- How much experience do they have?
From broad questions like these, you can begin to narrow down to more specific and open-ended questions.
Step three: The interview
If at all possible, arrange to conduct the interview at the subject’s workplace. It will make them more comfortable, and you can write about their surroundings.
- Begin the interview with some small talk in order to give both of you the chance to get comfortable with one another
- Develop rapport that will make the interview easier for both of you.
- Ask open-ended questions
- Keep the conversation moving
- Stay on topic
- The more silence in the room, the more honest the answer.
- If an interesting subject comes up that is related to your research, ask a follow-up or an additional question about it.
- Ask if you can stay in contact with your interview subject in case there are any additional questions you have.
Step four: Incorporating the interview
When picking the material out of your interview, remember that people rarely speak perfectly. There will be many slang words and pauses that you can take out, as long as it does not change the meaning of the material you are using.
As you introduce your interview in the paper, start with a transition such as “according to” or other attributions. You should also be specific to the type of interview you are working with. This way, you will build a stronger ethos in your paper .
The body of your essay should clearly set up the quote or paraphrase you use from the interview responses,. Be careful not to stick a quote from the interview into the body of your essay because it sounds good. When deciding what to quote in your paper, think about what dialogue from the interview would add the most color to your interview. Quotes that illustrate what your interviewer sounded like, or what their personality is are always the best quotes to choose from.
Once you have done that, proofread your essay. Make sure the quotes you used don’t make up the majority of your paper. The interview quotes are supposed to support your argument; you are not supposed to support the interview.
For example, let’s say that you are arguing that free education is better than not. For your argument, you interview a local politician who is on your side of the argument. Rather than using a large quote that explains the stance of both sides, and why the politician chose this side, your quote is there to support the information you’ve already given. Whatever the politician says should prove what you argue, and not give new information.
Step five: Examples of citing your interviews
Smith, Jane. Personal interview. 19 May 2018.
(E. Robbins, personal communication, January 4, 2018).
Smith also claimed that many of her students had difficulties with APA style (personal communication, November 3, 2018).
Reference list
Daly, C. & Leighton W. (2017). Interviewing a Source: Tips. Journalists Resource.
Driscoll, D. (2018 ). Interviewing. Purdue University
Hayden, K. (2012). How to Conduct an Interview to Write a Paper . Bright Hub Education, Bright Hub Inc.
Hose, C. (2017). How to Incorporate Interviews into Essays. Leaf Group Education.
Magnesi, J. (2017). How to Interview Someone for an Article or Research Paper. Career Trend, Leaf group Media.
Qualitative Research 101: Interviewing
5 Common Mistakes To Avoid When Undertaking Interviews
By: David Phair (PhD) and Kerryn Warren (PhD) | March 2022
Undertaking interviews is potentially the most important step in the qualitative research process. If you don’t collect useful, useable data in your interviews, you’ll struggle through the rest of your dissertation or thesis. Having helped numerous students with their research over the years, we’ve noticed some common interviewing mistakes that first-time researchers make. In this post, we’ll discuss five costly interview-related mistakes and outline useful strategies to avoid making these.
Overview: 5 Interviewing Mistakes
- Not having a clear interview strategy /plan
- Not having good interview techniques /skills
- Not securing a suitable location and equipment
- Not having a basic risk management plan
- Not keeping your “ golden thread ” front of mind
1. Not having a clear interview strategy
The first common mistake that we’ll look at is that of starting the interviewing process without having first come up with a clear interview strategy or plan of action. While it’s natural to be keen to get started engaging with your interviewees, a lack of planning can result in a mess of data and inconsistency between interviews.
There are several design choices to decide on and plan for before you start interviewing anyone. Some of the most important questions you need to ask yourself before conducting interviews include:
- What are the guiding research aims and research questions of my study?
- Will I use a structured, semi-structured or unstructured interview approach?
- How will I record the interviews (audio or video)?
- Who will be interviewed and by whom ?
- What ethics and data law considerations do I need to adhere to?
- How will I analyze my data?
Let’s take a quick look at some of these.
The core objective of the interviewing process is to generate useful data that will help you address your overall research aims. Therefore, your interviews need to be conducted in a way that directly links to your research aims, objectives and research questions (i.e. your “golden thread”). This means that you need to carefully consider the questions you’ll ask to ensure that they align with and feed into your golden thread. If any question doesn’t align with this, you may want to consider scrapping it.
Another important design choice is whether you’ll use an unstructured, semi-structured or structured interview approach . For semi-structured interviews, you will have a list of questions that you plan to ask and these questions will be open-ended in nature. You’ll also allow the discussion to digress from the core question set if something interesting comes up. This means that the type of information generated might differ a fair amount between interviews.
Contrasted to this, a structured approach to interviews is more rigid, where a specific set of closed questions is developed and asked for each interviewee in exactly the same order. Closed questions have a limited set of answers, that are often single-word answers. Therefore, you need to think about what you’re trying to achieve with your research project (i.e. your research aims) and decided on which approach would be best suited in your case.
It is also important to plan ahead with regards to who will be interviewed and how. You need to think about how you will approach the possible interviewees to get their cooperation, who will conduct the interviews, when to conduct the interviews and how to record the interviews. For each of these decisions, it’s also essential to make sure that all ethical considerations and data protection laws are taken into account.
Finally, you should think through how you plan to analyze the data (i.e., your qualitative analysis method) generated by the interviews. Different types of analysis rely on different types of data, so you need to ensure you’re asking the right types of questions and correctly guiding your respondents.
Simply put, you need to have a plan of action regarding the specifics of your interview approach before you start collecting data. If not, you’ll end up drifting in your approach from interview to interview, which will result in inconsistent, unusable data.

2. Not having good interview technique
While you’re generally not expected to become you to be an expert interviewer for a dissertation or thesis, it is important to practice good interview technique and develop basic interviewing skills .
Let’s go through some basics that will help the process along.
Firstly, before the interview , make sure you know your interview questions well and have a clear idea of what you want from the interview. Naturally, the specificity of your questions will depend on whether you’re taking a structured, semi-structured or unstructured approach, but you still need a consistent starting point . Ideally, you should develop an interview guide beforehand (more on this later) that details your core question and links these to the research aims, objectives and research questions.
Before you undertake any interviews, it’s a good idea to do a few mock interviews with friends or family members. This will help you get comfortable with the interviewer role, prepare for potentially unexpected answers and give you a good idea of how long the interview will take to conduct. In the interviewing process, you’re likely to encounter two kinds of challenging interviewees ; the two-word respondent and the respondent who meanders and babbles. Therefore, you should prepare yourself for both and come up with a plan to respond to each in a way that will allow the interview to continue productively.
To begin the formal interview , provide the person you are interviewing with an overview of your research. This will help to calm their nerves (and yours) and contextualize the interaction. Ultimately, you want the interviewee to feel comfortable and be willing to be open and honest with you, so it’s useful to start in a more casual, relaxed fashion and allow them to ask any questions they may have. From there, you can ease them into the rest of the questions.
As the interview progresses , avoid asking leading questions (i.e., questions that assume something about the interviewee or their response). Make sure that you speak clearly and slowly , using plain language and being ready to paraphrase questions if the person you are interviewing misunderstands. Be particularly careful with interviewing English second language speakers to ensure that you’re both on the same page.
Engage with the interviewee by listening to them carefully and acknowledging that you are listening to them by smiling or nodding. Show them that you’re interested in what they’re saying and thank them for their openness as appropriate. This will also encourage your interviewee to respond openly.
Need a helping hand?
3. Not securing a suitable location and quality equipment
Where you conduct your interviews and the equipment you use to record them both play an important role in how the process unfolds. Therefore, you need to think carefully about each of these variables before you start interviewing.
Poor location: A bad location can result in the quality of your interviews being compromised, interrupted, or cancelled. If you are conducting physical interviews, you’ll need a location that is quiet, safe, and welcoming . It’s very important that your location of choice is not prone to interruptions (the workplace office is generally problematic, for example) and has suitable facilities (such as water, a bathroom, and snacks).
If you are conducting online interviews , you need to consider a few other factors. Importantly, you need to make sure that both you and your respondent have access to a good, stable internet connection and electricity. Always check before the time that both of you know how to use the relevant software and it’s accessible (sometimes meeting platforms are blocked by workplace policies or firewalls). It’s also good to have alternatives in place (such as WhatsApp, Zoom, or Teams) to cater for these types of issues.
Poor equipment: Using poor-quality recording equipment or using equipment incorrectly means that you will have trouble transcribing, coding, and analyzing your interviews. This can be a major issue , as some of your interview data may go completely to waste if not recorded well. So, make sure that you use good-quality recording equipment and that you know how to use it correctly.
To avoid issues, you should always conduct test recordings before every interview to ensure that you can use the relevant equipment properly. It’s also a good idea to spot check each recording afterwards, just to make sure it was recorded as planned. If your equipment uses batteries, be sure to always carry a spare set.

4. Not having a basic risk management plan
Many possible issues can arise during the interview process. Not planning for these issues can mean that you are left with compromised data that might not be useful to you. Therefore, it’s important to map out some sort of risk management plan ahead of time, considering the potential risks, how you’ll minimize their probability and how you’ll manage them if they materialize.
Common potential issues related to the actual interview include cancellations (people pulling out), delays (such as getting stuck in traffic), language and accent differences (especially in the case of poor internet connections), issues with internet connections and power supply. Other issues can also occur in the interview itself. For example, the interviewee could drift off-topic, or you might encounter an interviewee who does not say much at all.
You can prepare for these potential issues by considering possible worst-case scenarios and preparing a response for each scenario. For instance, it is important to plan a backup date just in case your interviewee cannot make it to the first meeting you scheduled with them. It’s also a good idea to factor in a 30-minute gap between your interviews for the instances where someone might be late, or an interview runs overtime for other reasons. Make sure that you also plan backup questions that could be used to bring a respondent back on topic if they start rambling, or questions to encourage those who are saying too little.
In general, it’s best practice to plan to conduct more interviews than you think you need (this is called oversampling ). Doing so will allow you some room for error if there are interviews that don’t go as planned, or if some interviewees withdraw. If you need 10 interviews, it is a good idea to plan for 15. Likely, a few will cancel , delay, or not produce useful data.

5. Not keeping your golden thread front of mind
We touched on this a little earlier, but it is a key point that should be central to your entire research process. You don’t want to end up with pages and pages of data after conducting your interviews and realize that it is not useful to your research aims . Your research aims, objectives and research questions – i.e., your golden thread – should influence every design decision and should guide the interview process at all times.
A useful way to avoid this mistake is by developing an interview guide before you begin interviewing your respondents. An interview guide is a document that contains all of your questions with notes on how each of the interview questions is linked to the research question(s) of your study. You can also include your research aims and objectives here for a more comprehensive linkage.
You can easily create an interview guide by drawing up a table with one column containing your core interview questions . Then add another column with your research questions , another with expectations that you may have in light of the relevant literature and another with backup or follow-up questions . As mentioned, you can also bring in your research aims and objectives to help you connect them all together. If you’d like, you can download a copy of our free interview guide here .
Recap: Qualitative Interview Mistakes
In this post, we’ve discussed 5 common costly mistakes that are easy to make in the process of planning and conducting qualitative interviews.
To recap, these include:
If you have any questions about these interviewing mistakes, drop a comment below. Alternatively, if you’re interested in getting 1-on-1 help with your thesis or dissertation , check out our dissertation coaching service or book a free initial consultation with one of our friendly Grad Coaches.

Psst... there’s more!
This post was based on one of our popular Research Bootcamps . If you're working on a research project, you'll definitely want to check this out ...
Submit a Comment Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
- Print Friendly
- Harvard Library
- Research Guides
- Faculty of Arts & Sciences Libraries
Library Support for Qualitative Research
- Interview Research
General Handbooks and Overviews
Qualitative research communities.
- Types of Interviews
- Recruiting & Engaging Participants
- Interview Questions
- Conducting Interviews
- Recording & Transcription
- Data Analysis
- Managing Interview Data
- Finding Extant Interviews
- Past Workshops on Interview Research
- Methodological Resources
- Remote & Virtual Fieldwork
- Data Management & Repositories
- Campus Access
- Interviews as a Method for Qualitative Research (video) This short video summarizes why interviews can serve as useful data in qualitative research.
- InterViews by Steinar Kvale Interviewing is an essential tool in qualitative research and this introduction to interviewing outlines both the theoretical underpinnings and the practical aspects of the process. After examining the role of the interview in the research process, Steinar Kvale considers some of the key philosophical issues relating to interviewing: the interview as conversation, hermeneutics, phenomenology, concerns about ethics as well as validity, and postmodernism. Having established this framework, the author then analyzes the seven stages of the interview process - from designing a study to writing it up.
- Practical Evaluation by Michael Quinn Patton Surveys different interviewing strategies, from, a) informal/conversational, to b) interview guide approach, to c) standardized and open-ended, to d) closed/quantitative. Also discusses strategies for wording questions that are open-ended, clear, sensitive, and neutral, while supporting the speaker. Provides suggestions for probing and maintaining control of the interview process, as well as suggestions for recording and transcription.
- The SAGE Handbook of Interview Research by Amir B. Marvasti (Editor); James A. Holstein (Editor); Jaber F. Gubrium (Editor); Karyn D. McKinney (Editor) The new edition of this landmark volume emphasizes the dynamic, interactional, and reflexive dimensions of the research interview. Contributors highlight the myriad dimensions of complexity that are emerging as researchers increasingly frame the interview as a communicative opportunity as much as a data-gathering format. The book begins with the history and conceptual transformations of the interview, which is followed by chapters that discuss the main components of interview practice. Taken together, the contributions to The SAGE Handbook of Interview Research: The Complexity of the Craft encourage readers simultaneously to learn the frameworks and technologies of interviewing and to reflect on the epistemological foundations of the interview craft.
- International Congress of Qualitative Inquiry They host an annual confrerence at the University of Illinois at Urbana-Champaign, which aims to facilitate the development of qualitative research methods across a wide variety of academic disciplines, among other initiatives.
- METHODSPACE An online home of the research methods community, where practicing researchers share how to make research easier.
- Social Research Association, UK The SRA is the membership organisation for social researchers in the UK and beyond. It supports researchers via training, guidance, publications, research ethics, events, branches, and careers.
- Social Science Research Council The SSRC administers fellowships and research grants that support the innovation and evaluation of new policy solutions. They convene researchers and stakeholders to share evidence-based policy solutions and incubate new research agendas, produce online knowledge platforms and technical reports that catalog research-based policy solutions, and support mentoring programs that broaden problem-solving research opportunities.
- << Previous: Taguette
- Next: Types of Interviews >>
Except where otherwise noted, this work is subject to a Creative Commons Attribution 4.0 International License , which allows anyone to share and adapt our material as long as proper attribution is given. For details and exceptions, see the Harvard Library Copyright Policy ©2021 Presidents and Fellows of Harvard College.

Written Online Interviews in Qualitative Social Research: On the Methodological Grounding of a New Research Practice
- Daniela Schiek Universität Hamburg
In this article I discuss whether asynchronous written online interviews (e.g., via e-mail or a web forum) can be conducted narratively and based on guidelines, or whether the potential of written interviews is only reserved for certain forms of qualitative procedures. For this purpose, I utilize an empirical study and discuss if qualitative interviews are dependent on situational presence for their respective research goals. It turns out that discursive dialogues work in qualitative written online interviews, while narrative monologues without an immediate counterpart do not function as well. The written medium can therefore be used on the one hand via guided interviews and on the other hand via ethnographic processes, provided the research topic suggests this.
Author Biography
Daniela schiek, universität hamburg.
Daniela SCHIEK (Dipl.-Soz., Dr. phil., habil.) ist wissenschaftliche Mitarbeiterin an der Universität Hamburg. Ihre Arbeitsschwerpunkte sind qualitative Methoden der Sozialforschung, soziale Ungleichheit, Lebenslaufsoziologie und Generationenforschung. Veröffentlichungen u.a.: "Generationen der Armut. Zur familialen Transmission wohlfahrtsstaatlicher Abhängigkeit" (Wiesbaden: Springer VS, 2019), mit Carsten G. Ullrich und Frerk Blome; "Forumsdiskussionen. Untersuchung zu einem neuen qualitativen Forschungsinstrument" (Berlin: de Gruyter Oldenbourg, 2019), mit Carsten G. ULLRICH.
- HTML (Deutsch)
- PDF (Deutsch)
How to Cite
- Endnote/Zotero/Mendeley (RIS)
Copyright (c) 2022 Daniela Schiek

This work is licensed under a Creative Commons Attribution 4.0 International License .
Most read articles by the same author(s)
- Daniela Schiek, Poverty Generations: The Biographical Family Interview as a Methodological Key to Research on the Transmission of Poverty , Forum Qualitative Sozialforschung / Forum: Qualitative Social Research: Vol. 18 No. 3 (2017)
- Daniela Schiek, Carsten G. Ullrich, Conference Report: Qualitative Online Inquiry , Forum Qualitative Sozialforschung / Forum: Qualitative Social Research: Vol. 16 No. 2 (2015): Researcher, Migrant, Woman: Methodological Implications of Multiple Positionalities in Migration Studies
Make a Submission
Current issue, information.
- For Readers
- For Authors
- For Librarians
Usage Statistics Information
We log anonymous usage statistics. Please read the privacy information for details.
Developed By
2000-2024 Forum Qualitative Sozialforschung / Forum: Qualitative Social Research (ISSN 1438-5627) Institut für Qualitative Forschung , Internationale Akademie Berlin gGmbH
Hosting: Center for Digital Systems , Freie Universität Berlin Funding 2023-2025 by the KOALA project
FQS received the Enter Award 2024 in the "Pioneering Achievement" category , funded by the German Federal Ministry of Education and Research (BMBF) and implemented by the think tank iRights.Lab.
Privacy Statement Accessibility Statement

Introduction to Research Methods
6 qualitative research and interviews.
So we’ve described doing a survey and collecting quantitative data. But not all questions can best be answered by a survey. A survey is great for understanding what people think (for example), but not why they think what they do. If your research is intending to understand the underlying motivations or reasons behind peoples actions, or to build a deeper understanding on the background of a subject, an interview may be the more appropriate data collection method.
Interviews are a method of data collection that consist of two or more people exchanging information through a structured process of questions and answers. Questions are designed by the researcher to thoughtfully collect in-depth information on a topic or set of topics as related to the central research question. Interviews typically occur in-person, although good interviews can also be conducted remotely via the phone or video conferencing. Unlike surveys, interviews give the opportunity to ask follow-up questions and thoughtfully engage with participants on the spot (rather than the anonymous and impartial format of survey research).
And surveys can be used in qualitative or quantitative research – though they’re more typically a qualitative technique. In-depth interviews , containing open-ended questions and structured by an interview guide . One can also do a standardized interview with closed-ended questions (i.e. answer options) that are structured by an interview schedule as part of quantitative research. While these are called interviews they’re far closer to surveys, so we wont cover them again in this chapter. The terms used for in-depth interviews we’ll cover in the next section.
6.1 Interviews
In-depth interviews allow participants to describe experiences in their own words (a primary strength of the interview format). Strong in-depth interviews will include many open-ended questions that allow participants to respond in their own words, share new ideas, and lead the conversation in different directions. The purpose of open-ended questions and in-depth interviews is to hear as much as possible in the person’s own voice, to collect new information and ideas, and to achieve a level of depth not possible in surveys or most other forms of data collection.
Typically, an interview guide is used to create a soft structure for the conversation and is an important preparation tool for the researcher. You can not go into an interview unprepared and just “wing it”; what the interview guide allows you to do is map out a framework, order of topics, and may include specific questions to use during the interview. Generally, the interview guide is thought of as just that — a guide to use in order to keep the interview focused. It is not set in stone and a skilled researcher can change the order of questions or topics in an interviews based on the organic conversation flow.
Depending on the experience and skill level of the researcher, an interview guide can be as simple as a list of topics to cover. However, for consistency and quality of research, the interviewer may want to take the time to at least practice writing out questions in advance to ensure that phrasing and word choices are as clear, objective, and focused as possible. It’s worth remembering that working out the wording of questions in advance allows researchers to ensure more consistency across interview. The interview guide below, taken from the wonderful and free textbook Principles of Sociological Inquiry , shows an interview guide that just has topics.

Alternatively, you can use a more detailed guide that lists out possible questions, as shown below. A more detailed guide is probably better for an interviewer that has less experience, or is just beginning to work on a given topic.

The purpose of an interview guide is to help ask effective questions and to support the process of acquiring the best possible data for your research. Topics and questions should be organized thematically, and in a natural progression that will allow the conversation to flow and deepen throughout the course of the interview. Often, researchers will attempt to memorize or partially memorize the interview guide, in order to be more fully present with the participant during the conversation.
6.2 Asking good Questions
Remember, the purposes of interviews is to go more in-depth with an individual than is possible with a generalized survey. For this reason, it is important to use the guide as a starting point but not to be overly tethered to it during the actual interview process. You may get stuck when respondents give you shorter answers than you expect, or don’t provide the type of depth that you need for your research. Often, you may want to probe for more specifics. Think about using follow up questions like “How does/did that affect you?” or “How does X make you feel?” and “Tell me about a time where X…”
For example, if I was researching the relationship between pets and mental health, some strong open-ended questions might be: * How does your pet typically make you feel when you wake up in the morning? * How does your pet generally affect your mood when you arrive home in the evening? * Tell me about a time when your pet had a significant impact on your emotional state.
Questions framed in this manner leave plenty of room for the respondent to answer in their own words, as opposed to leading and/or truncated questions, such as: * Does being with your pet make you happy? * After a bad day, how much does seeing your pet improve your mood? * Tell me about how important your pet is to your mental health.
These questions assume outcomes and will not result in high quality research. Researchers should always avoid asking leading questions that give away an expected answer or suggest particular responses. For instance, if I ask “we need to spend more on public schools, don’t you think?” the respondent is more likely to agree regardless of their own thoughts. Some wont, but humans generally have a strong natural desire to be agreeable. That’s why leaving your questions neutral and open so that respondents can speak to their experiences and views is critical.
6.3 Analyzing Interview Data
Writing good questions and interviewing respondents are just the first steps of the interview process. After these stages, the researcher still has a lot of work to do to collect usable data from the interview. The researcher must spend time coding and analyzing the interview to retrieve this data. Just doing an interview wont produce data. Think about how many conversations you have everyday, and none of those are leaving you swimming in data.
Hopefully you can record your interviews. Recording your interviews will allow you the opportunity to transcribe them word for word later. If you can’t record the interview you’ll need to take detailed notes so that you can reconstruct what you heard later. Do not trust yourself to “just remember” the conversation. You’re collecting data, precious data that you’re spending time and energy to collect. Treat it as important and valuable. Remember our description of the methodology section from Chapter 2, you need to maintain a chain of custody on your data. If you just remembered the interview, you could be accused of making up the results. Your interview notes and the recording become part of that chain of custody to prove to others that your interviews were real and that your results are accurate.
Assuming you recorded your interview, the first step in the analysis process is transcribing the interview. A transcription is a written record of every word in an interview. Transcriptions can either be completed by the researcher or by a hired worker, though it is good practice for the researcher to transcribe the interview him or herself. Researchers should keep the following points in mind regarding transcriptions: * The interview should take place in a quiet location with minimal background noise to produce a clear recording; * Transcribing interviews is a time-consuming process and may take two to three times longer than the actual interview; * Transcriptions provide a more precise record of the interview than hand written notes and allow the interviewer to focus during the interview.
After transcribing the interview, the next step is to analyze the responses. Coding is the main form of analysis used for interviews and involves studying a transcription to identify important themes. These themes are categorized into codes, which are words or phrases that denote an idea.
You’ll typically being with several codes in mind that are generated by key ideas you week seeking in the questions, but you can also being by using open coding to understand the results. An open coding process involves reading through the transcript multiple times and paying close attention to each line of the text to discover noteworthy concepts. During the open coding process, the researcher keeps an open mind to find any codes that may be relevant to the research topic.
After the open coding process is complete, focused coding can begin. Focused coding takes a closer look at the notes compiled during the open coding stage to merge common codes and define what the codes mean in the context of the research project.
Imagine a researcher is conducting interviews to learn about various people’s experiences of childhood in New Orleans. The following example shows several codes that this researcher extrapolated from an interview with one of their subjects.

6.4 Using interview data
The next chapter will address ways to identify people to interview, but most of the remainder of the book will address how to analyze quantitative data. That shouldn’t be taken as a sign that quantitative data is better, or that it’s easier to use interview data. Because in an interview the researcher must interpret the words of others it is often more challenging to identify your findings and clearly answer your research question. However, quantitative data is more common, and there are more different things you can do with it, so we spend a lot of the textbook focusing on it.
I’ll work through one more example of using interview data though. It takes a lot of practice to be a good and skilled interviewer. What I show below is a brief excerpt of an interview I did, and how that data was used in a resulting paper I wrote. These aren’t the only way you can use interview data, but it’s an example of what the intermediary and final product might look like.
The overall project these are drawn from was concerned with minor league baseball stadiums, but the specific part I’m pulling from here was studying the decline and rejuvenation of downtown around those stadiums in several cities. You’ll see that I’m using the words of the respondent fairly directly, because that’s my data. But I’m not just relying on one respondent and trusting them, I did a few dozen interviews in order to understand the commonalities in people’s perspectives to build a narrative around my research question.

Excerpt from Notes

Excerpt from Resulting Paper
How many interviews are necessary? It actually doesn’t take many. What you want to observe in your interviews is theoretical saturation , where the codes you use in the transcript begin to appear across conversations and groups. If different people disagree that’s fine, but what you want to understand is the commonalities across peoples perspectives. Most research on the subject says that with 8 interviews you’ll typically start to see a decline in new information gathered. That doesn’t mean you won’t get new words , but you’ll stop hearing completely unique perspectives or gain novel insights. At that point, where you’ve ‘heard it all before’ you can stop, because you’ve probably identified the answer to the questions you were trying to research.
6.5 Ensuring Anonymity
One significant ethical concern with interviews, that also applies to surveys, is making sure that respondents maintain anonymity. In either form of data collection you may be asking respondents deeply personal questions, that if exposed may cause legal, personal, or professional harm. Notice that in the excerpt of the paper above the respondents are only identified by an id I assigned (Louisville D) and their career, rather than their name. I can only include the excerpt of the interview notes above because there are no details that might lead to them being identified.
You may want to report details about a person to contextualize the data you gathered, but you should always ensure that no one can be identified from your research. For instance, if you were doing research on racism at large companies, you may want to preface people’s comments by their race, as there is a good chance that white and minority employees would feel differently about the issues. However, if you preface someones comments by saying they’re a minority manager, that may violate their anonymity. Even if you don’t state what company you did interviews with, that may be enough detail for their co-workers to identify them if there are few minority managers at the company. As such, always think long and hard about whether there is any way that the participation of respondents may be exposed.
6.6 Why not both?

We’ve discussed surveys and interviews as different methods the last two chapters, but they can also complement each other.
For instance, let’s say you’re curious to study people who change opinions on abortion, either going from support to opposition or vice versa. You could use a survey to understand the prevalence of changing opinions, i.e. what percentage of people in your city have changed their views. That would help to establish whether this is a prominent issue, or whether it’s a rare phenomenon. But it would be difficult to understand from the survey what makes people change their views. You could add an open ended question for anyone that said they changed their opinion, but many people won’t respond and few will provide the level of detail necessary to understand their motivations. Interviews with people that have changed their opinions would give you an opportunity to explore how their experiences and beliefs have changed in combination with their views towards abortion.
6.7 Summary
In the last two chapters we’ve discussed the two most prominent methods of data collection in the social sciences: surveys and interviews. What we haven’t discussed though is how to identify the people you’ll collect data from; that’s called a sampling strategy. In the next chapter
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Chapter 13: Interviews
Danielle Berkovic
Learning outcomes
Upon completion of this chapter, you should be able to:
- Understand when to use interviews in qualitative research.
- Develop interview questions for an interview guide.
- Understand how to conduct an interview.
What are interviews?
An interviewing method is the most commonly used data collection technique in qualitative research. 1 The purpose of an interview is to explore the experiences, understandings, opinions and motivations of research participants. 2 Interviews are conducted one-on-one with the researcher and the participant. Interviews are most appropriate when seeking to understand a participant’s subjective view of an experience and are also considered suitable for the exploration of sensitive topics.
What are the different types of interviews?
There are four main types of interviews:
- Key stakeholder: A key stakeholder interview aims to explore one issue in detail with a person of interest or importance concerning the research topic. 3 Key stakeholder interviews seek the views of experts on some cultural, political or health aspects of the community, beyond their personal beliefs or actions. An example of a key stakeholder is the Chief Health Officer of Victoria (Australia’s second-most populous state) who oversaw the world’s longest lockdowns in response to the COVID-19 pandemic.
- Dyad: A dyad interview aims to explore one issue in a level of detail with a dyad (two people). This form of interviewing is used when one participant of the dyad may need some support or is not wholly able to articulate themselves (e.g. people with cognitive impairment, or children). Independence is acknowledged and the interview is analysed as a unit. 4
- Narrative: A narrative interview helps individuals tell their stories, and prioritises their own perspectives and experiences using the language that they prefer. 5 This type of interview has been widely used in social research but is gaining prominence in health research to better understand person-centred care, for example, negotiating exercise and food abstinence whilst living with Type 2 diabetes. 6,7
- Life history: A life history interview allows the researcher to explore a person’s individual and subjective experiences within a history of the time framework. 8 Life history interviews challenge the researcher to understand how people’s current attitudes, behaviours and choices are influenced by previous experiences or trauma. Life history interviews have been conducted with Holocaust survivors 9 and youth who have been forcibly recruited to war. 10
Table 13.4 provides a summary of four studies, each adopting one of these types of interviews.
Interviewing techniques
There are two main interview techniques:
- Semi-structured: Semi-structured interviewing aims to explore a few issues in moderate detail, to expand the researcher’s knowledge at some level. 11 Semi-structured interviews give the researcher the advantage of remaining reasonably objective while enabling participants to share their perspectives and opinions. The researcher should create an interview guide with targeted open questions to direct the interview. As examples, semi-structured interviews have been used to extend knowledge of why women might gain excess weight during pregnancy, 12 and to update guidelines for statin uptake. 13
- In-depth: In-depth interviewing aims to explore a person’s subjective experiences and feelings about a particular topic. 14 In-depth interviews are often used to explore emotive (e.g. end-of-life care) 15 and complex (e.g. adolescent pregnancy) topics. 16 The researcher should create an interview guide with selected open questions to ask of the participant, but the participant should guide the direction of the interview more than in a semi-structured setting. In-depth interviews value participants’ lived experiences and are frequently used in phenomenology studies (as described in Chapter 6) .
When to use the different types of interview s
The type of interview a researcher uses should be determined by the study design, the research aims and objectives, and participant demographics. For example, if conducting a descriptive study, semi-structured interviews may be the best method of data collection. As explained in Chapter 5 , descriptive studies seek to describe phenomena, rather than to explain or interpret the data. A semi-structured interview, which seeks to expand upon some level of existing knowledge, will likely best facilitate this.
Similarly, if conducting a phenomenological study, in-depth interviews may be the best method of data collection. As described in Chapter 6 , the key concept of phenomenology is the individual. The emphasis is on the lived experience of that individual and the person’s sense-making of those experiences. Therefore, an in-depth interview is likely best placed to elicit that rich data.
While some interview types are better suited to certain study designs, there are no restrictions on the type of interview that may be used. For example, semi-structured interviews provide an excellent accompaniment to trial participation (see Chapter 11 about mixed methods), and key stakeholder interviews, as part of an action research study, can be used to define priorities, barriers and enablers to implementation.
How do I write my interview questions?
An interview aims to explore the experiences, understandings, opinions and motivations of research participants. The general rule is that the interviewee should speak for 80 per cent of the interview, and the interviewer should only be asking questions and clarifying responses, for about 20 per cent of the interview. This percentage may differ depending on the interview type; for example, a semi-structured interview involves the researcher asking more questions than in an in-depth interview. Still, to facilitate free-flowing responses, it is important to use open-ended language to encourage participants to be expansive in their responses. Examples of open-ended terms include questions that start with ‘who’, ‘how’ and ‘where’.
The researcher should avoid closed-ended questions that can be answered with yes or no, and limit conversation. For example, asking a participant ‘Did you have this experience?’ can elicit a simple ‘yes’, whereas asking them to ‘Describe your experience’, will likely encourage a narrative response. Table 13.1 provides examples of terminology to include and avoid in developing interview questions.
Table 13.1. Interview question formats to use and avoid
| Use | Avoid |
|---|---|
| Tell me about… | Do you think that… |
| What happened when… | Will you do this… |
| Why is this important? | Did you believe that… |
| How did you feel when…How do you… | Were there issues from your perspective… |
| What are the…What does... |
How long should my interview be?
There is no rule about how long an interview should take. Different types of interviews will likely run for different periods of time, but this also depends on the research question/s and the type of participant. For example, given that a semi-structured interview is seeking to expand on some previous knowledge, the interview may need no longer than 30 minutes, or up to one hour. An in-depth interview seeks to explore a topic in a greater level of detail and therefore, at a minimum, would be expected to last an hour. A dyad interview may be as short as 15 minutes (e.g. if the dyad is a person with dementia and a family member or caregiver) or longer, depending on the pairing.
Designing your interview guide
To figure out what questions to ask in an interview guide, the researcher may consult the literature, speak to experts (including people with lived experience) about the research and draw on their current knowledge. The topics and questions should be mapped to the research question/s, and the interview guide should be developed well in advance of commencing data collection. This enables time and opportunity to pilot-test the interview guide. The pilot interview provides an opportunity to explore the language and clarity of questions, the order and flow of the guide and to determine whether the instructions are clear to participants both before and after the interview. It can be beneficial to pilot-test the interview guide with someone who is not familiar with the research topic, to make sure that the language used is easily understood (and will be by participants, too). The study design should be used to determine the number of questions asked and the duration of the interview should guide the extent of the interview guide. The participant type may also determine the extent of the interview guide; for example, clinicians tend to be time-poor and therefore shorter, focused interviews are optimal. An interview guide is also likely to be shorter for a descriptive study than a phenomenological or ethnographic study, given the level of detail required. Chapter 5 outlined a descriptive study in which participants who had undergone percutaneous coronary intervention were interviewed. The interview guide consisted of four main questions and subsequent probing questions, linked to the research questions (see Table 13.2). 17
Table 13.2. Interview guide for a descriptive study
| Research question | Open questions | Probing questions and topics |
|---|---|---|
| How does the patient feel, physically and psychologically, after their procedure? | From your perspective, what would be considered a successful outcome of the procedure? | Did the procedure meet your expectations? How do you define whether the procedure was successful? |
| How did you feel after the procedure?
| How did you feel one week after the procedure and how does that compare with how you feel now? | |
| How does the patient function after their procedure? | After your procedure, tell me about your ability to do your daily activities? | Prompt for activities including gardening, housework, personal care, work-related and family-related tasks.Did you attend cardiac rehabilitation? Can you tell us about your experience of cardiac rehabilitation? What effect has medication had on your recovery?
|
| What are the long-term effects of the procedure? | What, if any, lifestyle changes have you made since your procedure? |
Table 13.3 is an example of a larger and more detailed interview guide, designed for the qualitative component of a mixed-methods study aiming to examine the work and financial effects of living with arthritis as a younger person. The questions are mapped to the World Health Organization’s International Classification of Functioning, Disability, and Health, which measures health and disability at individual and population levels. 18
Table 13.3. Detailed interview guide
| Research questions | Open questions | Probing questions |
|---|---|---|
| How do young people experience their arthritis diagnosis? | Tell me about your experience of being diagnosed with arthritis.How did being diagnosed with arthritis make you feel?Tell me about your experience of arthritis flare ups what do they feel like?What impacts arthritis flare ups or feeling like your arthritis is worse?What circumstances lead to these feelings?Based on your experience, what do you think causes symptoms of arthritis to become worse? | When were you diagnosed with arthritis?What type of arthritis were you diagnosed with?Does anyone else in your family have arthritis? What relation are they to you? |
| What are the work impacts of arthritis on younger people? | What is your field of work, and how long have you been in this role?How frequently do you work (full-time/part-time/casual)? | How has arthritis affected your work-related demands or career? How so?Has arthritis led you to reconsider your career? How so?Has arthritis affected your usual working hours each week? How so?How have changes to work or career because of your arthritis impacted other areas of life, i.e. mental health or family role? |
| What are the financial impacts of living with arthritis as a younger person? | Has your arthritis led to any financial concerns? | Financial concerns pertaining to:• Direct costs: rheumatologist, prescribed and non-prescribed medications (as well as supplements), allied health costs (rheumatology, physiotherapy, chiropractic, osteopathy, myotherapy), Pilates, and gym/personal trainer fees, complementary therapies.• Indirect costs: workplace absenteeism, productivity, loss of wages, informal care, cost of different types of insurance: health insurance (joint replacements) |
It is important to create an interview guide, for the following reasons:
- The researcher should be familiar with their research questions.
- Using an interview guide will enable the incorporation of feedback from the piloting process.
- It is difficult to predict how participants will respond to interview questions. They may answer in a way that is anticipated or they may provide unanticipated insights that warrant follow-up. An interview guide (a physical or digital copy) enables the researcher to note these answers and follow-up with appropriate inquiry.
- Participants will likely have provided heterogeneous answers to certain questions. The interview guide enables the researcher to note similarities and differences across various interviews, which may be important in data analysis.
- Even experienced qualitative researchers get nervous before an interview! The interview guide provides a safety net if the researcher forgets their questions or needs to anticipate the next question.
Setting up the interview
In the past, most interviews were conducted in person or by telephone. Emerging technologies promote easier access to research participation (e.g. by people living in rural or remote communities, or for people with mobility limitations). Even in metropolitan settings, many interviews are now conducted electronically (e.g. using videoconferencing platforms). Regardless of your interview setting, it is essential that the interview environment is comfortable for the participant. This process can begin as soon as potential participants express interest in your research. Following are some tips from the literature and our own experiences of leading interviews:
- Answer questions and set clear expectations . Participating in research is not an everyday task. People do not necessarily know what to expect during a research interview, and this can be daunting. Give people as much information as possible, answer their questions about the research and set clear expectations about what the interview will entail and how long it is expected to last. Let them know that the interview will be recorded for transcription and analysis purposes. Consider sending the interview questions a few days before the interview. This gives people time and space to reflect on their experiences, consider their responses to questions and to provide informed consent for their participation.
- Consider your setting . If conducting the interview in person, consider the location and room in which the interview will be held. For example, if in a participant’s home, be mindful of their private space. Ask if you should remove your shoes before entering their home. If they offer refreshments (which in our experience many participants do), accept it with gratitude if possible. These considerations apply beyond the participant’s home; if using a room in an office setting, consider privacy and confidentiality, accessibility and potential for disruption. Consider the temperature as well as the furniture in the room, who may be able to overhear conversations and who may walk past. Similarly, if interviewing by phone or online, take time to assess the space, and if in a house or office that is not quiet or private, use headphones as needed.
- Build rapport. The research topic may be important to participants from a professional perspective, or they may have deep emotional connections to the topic of interest. Regardless of the nature of the interview, it is important to remember that participants are being asked to open up to an interviewer who is likely to be a stranger. Spend some time with participants before the interview, to make sure that they are comfortable. Engage in some general conversation, and ask if they have any questions before you start. Remember that it is not a normal part of someone’s day to participate in research. Make it an enjoyable and/or meaningful experience for them, and it will enhance the data that you collect.
- Let participants guide you. Oftentimes, the ways in which researchers and participants describe the same phenomena are different. In the interview, reflect the participant’s language. Make sure they feel heard and that they are willing and comfortable to speak openly about their experiences. For example, our research involves talking to older adults about their experience of falls. We noticed early in this research that participants did not use the word ‘fall’ but would rather use terms such as ‘trip’, ‘went over’ and ‘stumbled’. As interviewers we adopted the participant’s language into our questions.
- Listen consistently and express interest. An interview is more complex than a simple question-and-answer format. The best interview data comes from participants feeling comfortable and confident to share their stories. By the time you are completing the 20th interview, it can be difficult to maintain the same level of concentration as with the first interview. Try to stay engaged: nod along with your participants, maintain eye contact, murmur in agreement and sympathise where warranted.
- The interviewer is both the data collector and the data collection instrument. The data received is only as good as the questions asked. In qualitative research, the researcher influences how participants answer questions. It is important to remain reflexive and aware of how your language, body language and attitude might influence the interview. Being rested and prepared will enhance the quality of the questions asked and hence the data collected.
- Avoid excessive use of ‘why’. It can be challenging for participants to recall why they felt a certain way or acted in a particular manner. Try to avoid asking ‘why’ questions too often, and instead adopt some of the open language described earlier in the chapter.
After your interview
When you have completed your interview, thank the participant and let them know they can contact you if they have any questions or follow-up information they would like to provide. If the interview has covered sensitive topics or the participant has become distressed throughout the interview, make sure that appropriate referrals and follow-up are provided (see section 6).
Download the recording from your device and make sure it is saved in a secure location that can only be accessed by people on the approved research team (see Chapters 35 and 36).
It is important to know what to do immediately after each interview is completed. Interviews should be transcribed – that is, reproduced verbatim for data analysis. Transcribing data is an important step in the process of analysis, but it is very time-consuming; transcribing a 60-minute interview can take up to 8 hours. Data analysis is discussed in Section 4.
Table 13.4. Examples of the four types of interviews
| Title | ||||
|---|---|---|---|---|
| CC Licence | ||||
| First author and year | Cuthbertson, 2019 | Bannon, 2021 | McGranahan, 2020 | Gutierrez-Garcia, 2021 |
| Interview type | Key stakeholder | Dyad | Narrative | Life history |
| Interview guide | Appendix A | eAppendix Supplement | Not provided, but the text states that ‘qualitative semi-structured narrative interviews’ were conducted.’ [methods] | Not provided, but the text states that ‘an open and semi-structured question guide was designed for use.' [methods] |
| Study design | Convergent mixed-methods study | Qualitative dyadic study | Narrative interview study | Life history and lifeline techniques |
| Number of participants | 30Key stakeholders were emergency management or disaster healthcare practitioners, academics specialising in disaster management in the Oceania region, and policy managers. | 23 dyads | 28 | 7 |
| Aim | ‘To investigate threats to the health and well-being of societies associated with disaster impact in Oceania.’ [abstract] | ‘To explore the lived experiences of couples managing young-onset dementia using an integrated dyadic coping model.’[abstract] | ‘To explore the experiences and views of people with psychotic experiences who have not received any treatment or other support from mental health services for the past 5 years.’ [abstract] | ‘To analyse the use of life histories and lifelines in the study of female genital mutilation in the context of cross-cultural research in participants with different languages.’ [abstract] |
| Country | Australia, Fiji, Indonesia, Aotearoa New Zealand, Timor Leste and Tonga | United States | England | Spain |
| Length of interview | 45–60 minutes | 60 minutes | 40-120 minutes | 3 sessionsSession 1: life history interviewSession 2: Lifeline activity where participants used drawings to complement or enhance their interviewSession 3: The researchers and participants worked together to finalise the lifeline. The life history interviews ran for 40 – 60 minutes. The timing for sessions 2 and 3 is not provided. |
| Sample of interview questions from interview guide | 1. What do you believe are the top five disaster risks or threats in the Oceania region today?2. What disaster risks do you believe are emerging in the Oceania region over the next decade?3. Why do you think these are risks?4. What are the drivers of these risks?5. Do you have any suggestions on how we can improve disaster risk assessment?6. Are the current disaster risk plans and practices suited to the future disaster risks? If not, why? If not, what do you think needs to be done to improve them?7. What are the key areas of disaster practice that can enhance future community resilience to disaster risk?8. What are the barriers or inhibitors to facilitating this practice?9. What are the solutions or facilitators to enhancing community resilience?[Appendix A]
| 1. We like to start by learning more about what you each first noticed that prompted the evaluations you went through to get to the diagnosis.• Can you each tell me about the earliest symptoms you noticed?2. What are the most noticeable or troubling symptoms that you have experienced since the time of diagnosis?• How have your changes in functioning impacted you?• Emotionally, how do you feel about your symptoms and the changes in functioning you are experiencing?3. Are you open with your friends and family about the diagnosis?• Have you experienced any stigma related to your diagnosis?4. What is your understanding of the diagnosis?• What is your understanding about the how this condition will affect you both in the future? How are you getting information about this diagnosis?[eAppendix Supplement]
| Not provided. | Not provided. |
| Analysis | Thematic analysis guided by The Hazard and Peril Glossary for describing and categorising disasters applied by the Centre for Research on the Epidemiology of Disasters Emergency Events Database | Thematic analysis guided by the Dyadic Coping Theoretical Framework | Inductive thematic analysis outlined by Braun and Clarke. | Phenomenological method proposed by Giorgi (sense of the whole):1. Reading the entire description to obtain a general sense of the discourse2. The researcher goes back to the beginning and reads the text again, with the aim of distinguishing the meaning units by separating the perspective of the phenomenon of interest3. The researcher expresses the contents of the units of meaning more clearly by creating categories4. The researcher synthesises the units and categories of meaning into a consistent statement that takes into account the participant’s experience and language. |
| Main themes | 1. Climate change is observed as a contemporary and emerging disaster risk2. Risk is contextual to the different countries, communities and individuals in Oceania.3. Human development trajectories and their impact, along with perceptions of a changing world, are viewed as drivers of current and emerging risks.4. Current disaster risk plans and practices are not suited to future disaster risks.5. Increased education and education of risk and risk assessment at a local level to empower community risk ownership.[Results, Box 1] | 1. Stress communication2. Positive individual dyadic coping3. Positive conjoint dyadic coping4. Negative individual dyadic coping5. Negative conjoint dyadic coping[Abstract] | 1. Perceiving psychosis as positive2. Making sense of psychotic experiences3. Finding sources of strength4. Negative past experiences of mental health services5. Positive past experiences with individual clinicians[Abstract] | 1. Important moments and their relationship with female genital mutilation2. The ritual knife: how sharp or blunt it is at different stages, where and how women are subsequently held as a result3. Changing relationships with family: how being subject to female genital mutilation changed relationships with mothers4. Female genital mutilation increases the risk of future childbirth complications which change relationships with family and healthcare systems5. Managing experiences with early exposure to physical and sexual violence across the lifespan. |
Interviews are the most common data collection technique in qualitative research. There are four main types of interviews; the one you choose will depend on your research question, aims and objectives. It is important to formulate open-ended interview questions that are understandable and easy for participants to answer. Key considerations in setting up the interview will enhance the quality of the data obtained and the experience of the interview for the participant and the researcher.
- Gill P, Stewart K, Treasure E, Chadwick B. Methods of data collection in qualitative research: interviews and focus groups. Br Dent J . 2008;204(6):291-295. doi:10.1038/bdj.2008.192
- DeJonckheere M, Vaughn LM. Semistructured interviewing in primary care research: a balance of relationship and rigour. Fam Med Community Health . 2019;7(2):e000057. doi:10.1136/fmch-2018-000057
- Nyanchoka L, Tudur-Smith C, Porcher R, Hren D. Key stakeholders’ perspectives and experiences with defining, identifying and displaying gaps in health research: a qualitative study. BMJ Open . 2020;10(11):e039932. doi:10.1136/bmjopen-2020-039932
- Morgan DL, Ataie J, Carder P, Hoffman K. Introducing dyadic interviews as a method for collecting qualitative data. Qual Health Res . 2013;23(9):1276-84. doi:10.1177/1049732313501889
- Picchi S, Bonapitacola C, Borghi E, et al. The narrative interview in therapeutic education. The diabetic patients’ point of view. Acta Biomed . Jul 18 2018;89(6-S):43-50. doi:10.23750/abm.v89i6-S.7488
- Stuij M, Elling A, Abma T. Negotiating exercise as medicine: Narratives from people with type 2 diabetes. Health (London) . 2021;25(1):86-102. doi:10.1177/1363459319851545
- Buchmann M, Wermeling M, Lucius-Hoene G, Himmel W. Experiences of food abstinence in patients with type 2 diabetes: a qualitative study. BMJ Open . 2016;6(1):e008907. doi:10.1136/bmjopen-2015-008907
- Jessee E. The Life History Interview. Handbook of Research Methods in Health Social Sciences . 2018:1-17:Chapter 80-1.
- Sheftel A, Zembrzycki S. Only Human: A Reflection on the Ethical and Methodological Challenges of Working with “Difficult” Stories. The Oral History Review . 2019;37(2):191-214. doi:10.1093/ohr/ohq050
- Harnisch H, Montgomery E. “What kept me going”: A qualitative study of avoidant responses to war-related adversity and perpetration of violence by former forcibly recruited children and youth in the Acholi region of northern Uganda. Soc Sci Med . 2017;188:100-108. doi:10.1016/j.socscimed.2017.07.007
- Ruslin., Mashuri S, Rasak MSA, Alhabsyi M, Alhabsyi F, Syam H. Semi-structured Interview: A Methodological Reflection on the Development of a Qualitative Research Instrument in Educational Studies. IOSR-JRME . 2022;12(1):22-29. doi:10.9790/7388-1201052229
- Chang T, Llanes M, Gold KJ, Fetters MD. Perspectives about and approaches to weight gain in pregnancy: a qualitative study of physicians and nurse midwives. BMC Pregnancy & Childbirth . 2013;13(47)doi:10.1186/1471-2393-13-47
- DeJonckheere M, Robinson CH, Evans L, et al. Designing for Clinical Change: Creating an Intervention to Implement New Statin Guidelines in a Primary Care Clinic. JMIR Hum Factors . 2018;5(2):e19. doi:10.2196/humanfactors.9030
- Knott E, Rao AH, Summers K, Teeger C. Interviews in the social sciences. Nature Reviews Methods Primers . 2022;2(1)doi:10.1038/s43586-022-00150-6
- Bergenholtz H, Missel M, Timm H. Talking about death and dying in a hospital setting – a qualitative study of the wishes for end-of-life conversations from the perspective of patients and spouses. BMC Palliat Care . 2020;19(1):168. doi:10.1186/s12904-020-00675-1
- Olorunsaiye CZ, Degge HM, Ubanyi TO, Achema TA, Yaya S. “It’s like being involved in a car crash”: teen pregnancy narratives of adolescents and young adults in Jos, Nigeria. Int Health . 2022;14(6):562-571. doi:10.1093/inthealth/ihab069
- Ayton DR, Barker AL, Peeters G, et al. Exploring patient-reported outcomes following percutaneous coronary intervention: A qualitative study. Health Expect . 2018;21(2):457-465. doi:10.1111/hex.12636
- World Health Organization. International Classification of Functioning, Disability and Health (ICF). WHO. https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health#:~:text=ICF%20is%20the%20WHO%20framework,and%20measure%20health%20and%20disability.
- Cuthbertson J, Rodriguez-Llanes JM, Robertson A, Archer F. Current and Emerging Disaster Risks Perceptions in Oceania: Key Stakeholders Recommendations for Disaster Management and Resilience Building. Int J Environ Res Public Health . 2019;16(3)doi:10.3390/ijerph16030460
- Bannon SM, Grunberg VA, Reichman M, et al. Thematic Analysis of Dyadic Coping in Couples With Young-Onset Dementia. JAMA Netw Open . 2021;4(4):e216111. doi:10.1001/jamanetworkopen.2021.6111
- McGranahan R, Jakaite Z, Edwards A, Rennick-Egglestone S, Slade M, Priebe S. Living with Psychosis without Mental Health Services: A Narrative Interview Study. BMJ Open . 2021;11(7):e045661. doi:10.1136/bmjopen-2020-045661
- Gutiérrez-García AI, Solano-Ruíz C, Siles-González J, Perpiñá-Galvañ J. Life Histories and Lifelines: A Methodological Symbiosis for the Study of Female Genital Mutilation. Int J Qual Methods . 2021;20doi:10.1177/16094069211040969
Qualitative Research – a practical guide for health and social care researchers and practitioners Copyright © 2023 by Danielle Berkovic is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License , except where otherwise noted.
Share This Book
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, generate accurate citations for free.
- Knowledge Base
Methodology
- Structured Interview | Definition, Guide & Examples
Structured Interview | Definition, Guide & Examples
Published on January 27, 2022 by Tegan George and Julia Merkus. Revised on June 22, 2023.
A structured interview is a data collection method that relies on asking questions in a set order to collect data on a topic. It is one of four types of interviews .
In research, structured interviews are often quantitative in nature. They can also be used in qualitative research if the questions are open-ended, but this is less common.
While structured interviews are often associated with job interviews, they are also common in marketing, social science, survey methodology, and other research fields.
- Semi-structured interviews : A few questions are predetermined, whereas the other questions aren’t planned.
- Unstructured interviews : None of the questions are predetermined.
- Focus group interviews : The questions are presented to a group instead of one individual.
Table of contents
What is a structured interview, when to use a structured interview, advantages of structured interviews, disadvantages of structured interviews, structured interview questions, how to conduct a structured interview, how to analyze a structured interview, presenting your results, other interesting articles, frequently asked questions about structured interviews.
Structured interviews are the most systematized type of interview. In contrast to semi-structured or unstructured interviews, the interviewer uses predetermined questions in a set order.
Structured interviews are often closed-ended. They can be dichotomous, which means asking participants to answer “yes” or “no” to each question, or multiple-choice. While open-ended structured interviews do exist, they are less common.
Asking set questions in a set order allows you to easily compare responses between participants in a uniform context. This can help you see patterns and highlight areas for further research, and it can be a useful explanatory or exploratory research tool.
Structured interviews are best used when:
- You already have a very clear understanding of your topic, so you possess a baseline for designing strong structured questions.
- You are constrained in terms of time or resources and need to analyze your data efficiently.
- Your research question depends on strong parity between participants, with environmental conditions held constant.
A structured interview is straightforward to conduct and analyze. Asking the same set of questions mitigates potential biases and leads to fewer ambiguities in analysis. It is an undertaking you can likely handle as an individual, provided you remain organized.
Differences between different types of interviews
Make sure to choose the type of interview that suits your research best. This table shows the most important differences between the four types.
| Fixed questions | ||||
|---|---|---|---|---|
| Fixed order of questions | ||||
| Fixed number of questions | ||||
| Option to ask additional questions |
Reduced bias
Increased credibility, reliability and validity, simple, cost-effective and efficient, formal in nature, limited flexibility, limited scope.
It can be difficult to write structured interview questions that approximate exactly what you are seeking to measure. Here are a few tips for writing questions that contribute to high internal validity :
- Define exactly what you want to discover prior to drafting your questions. This will help you write questions that really zero in on participant responses.
- Avoid jargon, compound sentences, and complicated constructions.
- Be as clear and concise as possible, so that participants can answer your question immediately.
- Do you think that employers should provide free gym memberships?
- Did any of your previous employers provide free memberships?
- Does your current employer provide a free membership?
- a) 1 time; b) 2 times; c) 3 times; d) 4 or more times
- Do you enjoy going to the gym?
Structured interviews are among the most straightforward research methods to conduct and analyze. Once you’ve determined that they’re the right fit for your research topic , you can proceed with the following steps.
Step 1: Set your goals and objectives
Start with brainstorming some guiding questions to help you conceptualize your research question, such as:
- What are you trying to learn or achieve from a structured interview?
- Why are you choosing a structured interview as opposed to a different type of interview, or another research method?
If you have satisfying reasoning for proceeding with a structured interview, you can move on to designing your questions.
Step 2: Design your questions
Pay special attention to the order and wording of your structured interview questions . Remember that in a structured interview they must remain the same. Stick to closed-ended or very simple open-ended questions.
Step 3: Assemble your participants
Depending on your topic, there are a few sampling methods you can use, such as:
- Voluntary response sampling : For example, posting a flyer on campus and finding participants based on responses
- Convenience sampling of those who are most readily accessible to you, such as fellow students at your university
- Stratified sampling of a particular age, race, ethnicity, gender identity, or other characteristic of interest to you
- Judgment sampling of a specific set of participants that you already know you want to include
Step 4: Decide on your medium
Determine whether you will be conducting your interviews in person or whether your interview will take pen-and-paper format. If conducted live, you need to decide if you prefer to talk with participants in person, over the phone, or via video conferencing.
Step 5: Conduct your interviews
As you conduct your interviews, be very careful that all conditions remain as constant as possible.
- Ask your questions in the same order, and try to moderate your tone of voice and any responses to participants as much as you can.
- Pay special attention to your body language (e.g., nodding, raising eyebrows), as this can bias responses.
After you’re finished conducting your interviews, it’s time to analyze your results.
- Assign each of your participants a number or pseudonym for organizational purposes.
- Transcribe the recordings manually or with the help of transcription software.
- Conduct a content or thematic analysis to look for categories or patterns of responses. In most cases, it’s also possible to conduct a statistical analysis to test your hypotheses .
Transcribing interviews
If you have audio-recorded your interviews, you will likely have to transcribe them prior to conducting your analysis. In some cases, your supervisor might ask you to add the transcriptions in the appendix of your paper.
First, you will have to decide whether to conduct verbatim transcription or intelligent verbatim transcription. Do pauses, laughter, or filler words like “umm” or “like” affect your analysis and research conclusions?
- If so, conduct verbatim transcription and include them.
- If not, conduct intelligent verbatim transcription, which excludes fillers and fixes any grammar issues, and is often easier to analyze.
The transcription process is a great opportunity for you to cleanse your data as well, spotting and resolving any inconsistencies or errors that come up as you listen.
Coding and analyzing structured interviews
After transcribing, it’s time to conduct your thematic or content analysis . This often involves “coding” words, patterns, or themes, separating them into categories for more robust analysis.
Due to the closed-ended nature of many structured interviews, you will most likely be conducting content analysis, rather than thematic analysis.
- You quantify the categories you chose in the coding stage by counting the occurrence of the words, phrases, subjects or concepts you selected.
- After coding, you can organize and summarize the data using descriptive statistics .
- Next, inferential statistics allows you to come to conclusions about your hypotheses and make predictions for future research.
When conducting content analysis, you can take an inductive or a deductive approach. With an inductive approach, you allow the data to determine your themes. A deductive approach is the opposite, and involves investigating whether your data confirm preconceived themes or ideas.
Content analysis has a systematic procedure that can easily be replicated , yielding high reliability to your results. However, keep in mind that while this approach reduces bias, it doesn’t eliminate it. Be vigilant about remaining objective here, even if your analysis does not confirm your hypotheses .
After your data analysis, the next step is to combine your findings into a research paper .
- Your methodology section describes how you collected the data (in this case, describing your structured interview process) and explains how you justify or conceptualize your analysis.
- Your discussion and results sections usually address each of your coded categories, describing each in turn, as well as how often they occurred.
If you conducted inferential statistics in addition to descriptive statistics, you would generally report the test statistic , p -value , and effect size in your results section. These values explain whether your results justify rejecting your null hypothesis and whether the result is practically significant .
You can then conclude with the main takeaways and avenues for further research.
Example of interview methodology for a research paper
Let’s say you are interested in healthcare on your campus. You attend a large public institution with a lot of international students, and you think there may be a difference in perceptions based on country of origin.
Specifically, you hypothesize that students coming from countries with single-payer or socialized healthcare will find US options less satisfying.
There is a large body of research available on this topic, so you decide to conduct structured interviews of your peers to see if there’s a difference between international students and local students.
You are a member of a large campus club that brings together international students and local students, and you send a message to the club to ask for volunteers.
Here are some questions you could ask:
- Do you find healthcare options on campus to be: excellent; good; fair; average; poor?
- Does your home country have socialized healthcare? Yes/No
- Are you on the campus healthcare plan? Yes/No
- Have you ever worried about your health insurance? Yes/No
- Have you ever had a serious health condition that insurance did not cover? Yes/No
- Have you ever been surprised or shocked by a medical bill? Yes/No
After conducting your interviews and transcribing your data, you can then conduct content analysis, coding responses into different categories. Since you began your research with the theory that international students may find US healthcare lacking, you would use the deductive approach to see if your hypotheses seem to hold true.
If you want to know more about statistics , methodology , or research bias , make sure to check out some of our other articles with explanations and examples.
- Student’s t -distribution
- Normal distribution
- Null and Alternative Hypotheses
- Chi square tests
- Confidence interval
- Quartiles & Quantiles
- Cluster sampling
- Stratified sampling
- Data cleansing
- Reproducibility vs Replicability
- Peer review
- Prospective cohort study
Research bias
- Implicit bias
- Cognitive bias
- Placebo effect
- Hawthorne effect
- Hindsight bias
- Affect heuristic
- Social desirability bias
A structured interview is a data collection method that relies on asking questions in a set order to collect data on a topic. They are often quantitative in nature. Structured interviews are best used when:
- You already have a very clear understanding of your topic. Perhaps significant research has already been conducted, or you have done some prior research yourself, but you already possess a baseline for designing strong structured questions.
- You are constrained in terms of time or resources and need to analyze your data quickly and efficiently.
More flexible interview options include semi-structured interviews , unstructured interviews , and focus groups .
The four most common types of interviews are:
- Structured interviews : The questions are predetermined in both topic and order.
- Semi-structured interviews : A few questions are predetermined, but other questions aren’t planned.
The interviewer effect is a type of bias that emerges when a characteristic of an interviewer (race, age, gender identity, etc.) influences the responses given by the interviewee.
There is a risk of an interviewer effect in all types of interviews , but it can be mitigated by writing really high-quality interview questions.
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the “Cite this Scribbr article” button to automatically add the citation to our free Citation Generator.
George, T. & Merkus, J. (2023, June 22). Structured Interview | Definition, Guide & Examples. Scribbr. Retrieved September 3, 2024, from https://www.scribbr.com/methodology/structured-interview/
Is this article helpful?

Tegan George
Other students also liked, semi-structured interview | definition, guide & examples, unstructured interview | definition, guide & examples, what is a focus group | step-by-step guide & examples, what is your plagiarism score.
Root out friction in every digital experience, super-charge conversion rates, and optimize digital self-service
Uncover insights from any interaction, deliver AI-powered agent coaching, and reduce cost to serve
Increase revenue and loyalty with real-time insights and recommendations delivered to teams on the ground
Know how your people feel and empower managers to improve employee engagement, productivity, and retention
Take action in the moments that matter most along the employee journey and drive bottom line growth
Whatever they’re are saying, wherever they’re saying it, know exactly what’s going on with your people
Get faster, richer insights with qual and quant tools that make powerful market research available to everyone
Run concept tests, pricing studies, prototyping + more with fast, powerful studies designed by UX research experts
Track your brand performance 24/7 and act quickly to respond to opportunities and challenges in your market
Explore the platform powering Experience Management
- Free Account
- Product Demos
- For Digital
- For Customer Care
- For Human Resources
- For Researchers
- Financial Services
- All Industries
Popular Use Cases
- Customer Experience
- Employee Experience
- Net Promoter Score
- Voice of Customer
- Customer Success Hub
- Product Documentation
- Training & Certification
- XM Institute
- Popular Resources
- Customer Stories
- Artificial Intelligence
Market Research
- Partnerships
- Marketplace
The annual gathering of the experience leaders at the world’s iconic brands building breakthrough business results, live in Salt Lake City.
- English/AU & NZ
- Español/Europa
- Español/América Latina
- Português Brasileiro
- REQUEST DEMO
- Experience Management
- Qualitative Research Interviews
Try Qualtrics for free
How to carry out great interviews in qualitative research.
11 min read An interview is one of the most versatile methods used in qualitative research. Here’s what you need to know about conducting great qualitative interviews.
What is a qualitative research interview?
Qualitative research interviews are a mainstay among q ualitative research techniques, and have been in use for decades either as a primary data collection method or as an adjunct to a wider research process. A qualitative research interview is a one-to-one data collection session between a researcher and a participant. Interviews may be carried out face-to-face, over the phone or via video call using a service like Skype or Zoom.
There are three main types of qualitative research interview – structured, unstructured or semi-structured.
- Structured interviews Structured interviews are based around a schedule of predetermined questions and talking points that the researcher has developed. At their most rigid, structured interviews may have a precise wording and question order, meaning that they can be replicated across many different interviewers and participants with relatively consistent results.
- Unstructured interviews Unstructured interviews have no predetermined format, although that doesn’t mean they’re ad hoc or unplanned. An unstructured interview may outwardly resemble a normal conversation, but the interviewer will in fact be working carefully to make sure the right topics are addressed during the interaction while putting the participant at ease with a natural manner.
- Semi-structured interviews Semi-structured interviews are the most common type of qualitative research interview, combining the informality and rapport of an unstructured interview with the consistency and replicability of a structured interview. The researcher will come prepared with questions and topics, but will not need to stick to precise wording. This blended approach can work well for in-depth interviews.
Free eBook: The qualitative research design handbook
What are the pros and cons of interviews in qualitative research?
As a qualitative research method interviewing is hard to beat, with applications in social research, market research, and even basic and clinical pharmacy. But like any aspect of the research process, it’s not without its limitations. Before choosing qualitative interviewing as your research method, it’s worth weighing up the pros and cons.
Pros of qualitative interviews:
- provide in-depth information and context
- can be used effectively when their are low numbers of participants
- provide an opportunity to discuss and explain questions
- useful for complex topics
- rich in data – in the case of in-person or video interviews , the researcher can observe body language and facial expression as well as the answers to questions
Cons of qualitative interviews:
- can be time-consuming to carry out
- costly when compared to some other research methods
- because of time and cost constraints, they often limit you to a small number of participants
- difficult to standardize your data across different researchers and participants unless the interviews are very tightly structured
- As the Open University of Hong Kong notes, qualitative interviews may take an emotional toll on interviewers
Qualitative interview guides
Semi-structured interviews are based on a qualitative interview guide, which acts as a road map for the researcher. While conducting interviews, the researcher can use the interview guide to help them stay focused on their research questions and make sure they cover all the topics they intend to.
An interview guide may include a list of questions written out in full, or it may be a set of bullet points grouped around particular topics. It can prompt the interviewer to dig deeper and ask probing questions during the interview if appropriate.
Consider writing out the project’s research question at the top of your interview guide, ahead of the interview questions. This may help you steer the interview in the right direction if it threatens to head off on a tangent.
Avoid bias in qualitative research interviews
According to Duke University , bias can create significant problems in your qualitative interview.
- Acquiescence bias is common to many qualitative methods, including focus groups. It occurs when the participant feels obliged to say what they think the researcher wants to hear. This can be especially problematic when there is a perceived power imbalance between participant and interviewer. To counteract this, Duke University’s experts recommend emphasizing the participant’s expertise in the subject being discussed, and the value of their contributions.
- Interviewer bias is when the interviewer’s own feelings about the topic come to light through hand gestures, facial expressions or turns of phrase. Duke’s recommendation is to stick to scripted phrases where this is an issue, and to make sure researchers become very familiar with the interview guide or script before conducting interviews, so that they can hone their delivery.
What kinds of questions should you ask in a qualitative interview?
The interview questions you ask need to be carefully considered both before and during the data collection process. As well as considering the topics you’ll cover, you will need to think carefully about the way you ask questions.
Open-ended interview questions – which cannot be answered with a ‘yes’ ‘no’ or ‘maybe’ – are recommended by many researchers as a way to pursue in depth information.
An example of an open-ended question is “What made you want to move to the East Coast?” This will prompt the participant to consider different factors and select at least one. Having thought about it carefully, they may give you more detailed information about their reasoning.
A closed-ended question , such as “Would you recommend your neighborhood to a friend?” can be answered without too much deliberation, and without giving much information about personal thoughts, opinions and feelings.
Follow-up questions can be used to delve deeper into the research topic and to get more detail from open-ended questions. Examples of follow-up questions include:
- What makes you say that?
- What do you mean by that?
- Can you tell me more about X?
- What did/does that mean to you?
As well as avoiding closed-ended questions, be wary of leading questions. As with other qualitative research techniques such as surveys or focus groups, these can introduce bias in your data. Leading questions presume a certain point of view shared by the interviewer and participant, and may even suggest a foregone conclusion.
An example of a leading question might be: “You moved to New York in 1990, didn’t you?” In answering the question, the participant is much more likely to agree than disagree. This may be down to acquiescence bias or a belief that the interviewer has checked the information and already knows the correct answer.
Other leading questions involve adjectival phrases or other wording that introduces negative or positive connotations about a particular topic. An example of this kind of leading question is: “Many employees dislike wearing masks to work. How do you feel about this?” It presumes a positive opinion and the participant may be swayed by it, or not want to contradict the interviewer.
Harvard University’s guidelines for qualitative interview research add that you shouldn’t be afraid to ask embarrassing questions – “if you don’t ask, they won’t tell.” Bear in mind though that too much probing around sensitive topics may cause the interview participant to withdraw. The Harvard guidelines recommend leaving sensitive questions til the later stages of the interview when a rapport has been established.
More tips for conducting qualitative interviews
Observing a participant’s body language can give you important data about their thoughts and feelings. It can also help you decide when to broach a topic, and whether to use a follow-up question or return to the subject later in the interview.
Be conscious that the participant may regard you as the expert, not themselves. In order to make sure they express their opinions openly, use active listening skills like verbal encouragement and paraphrasing and clarifying their meaning to show how much you value what they are saying.
Remember that part of the goal is to leave the interview participant feeling good about volunteering their time and their thought process to your research. Aim to make them feel empowered , respected and heard.
Unstructured interviews can demand a lot of a researcher, both cognitively and emotionally. Be sure to leave time in between in-depth interviews when scheduling your data collection to make sure you maintain the quality of your data, as well as your own well-being .
Recording and transcribing interviews
Historically, recording qualitative research interviews and then transcribing the conversation manually would have represented a significant part of the cost and time involved in research projects that collect qualitative data.
Fortunately, researchers now have access to digital recording tools, and even speech-to-text technology that can automatically transcribe interview data using AI and machine learning. This type of tool can also be used to capture qualitative data from qualitative research (focus groups,ect.) making this kind of social research or market research much less time consuming.
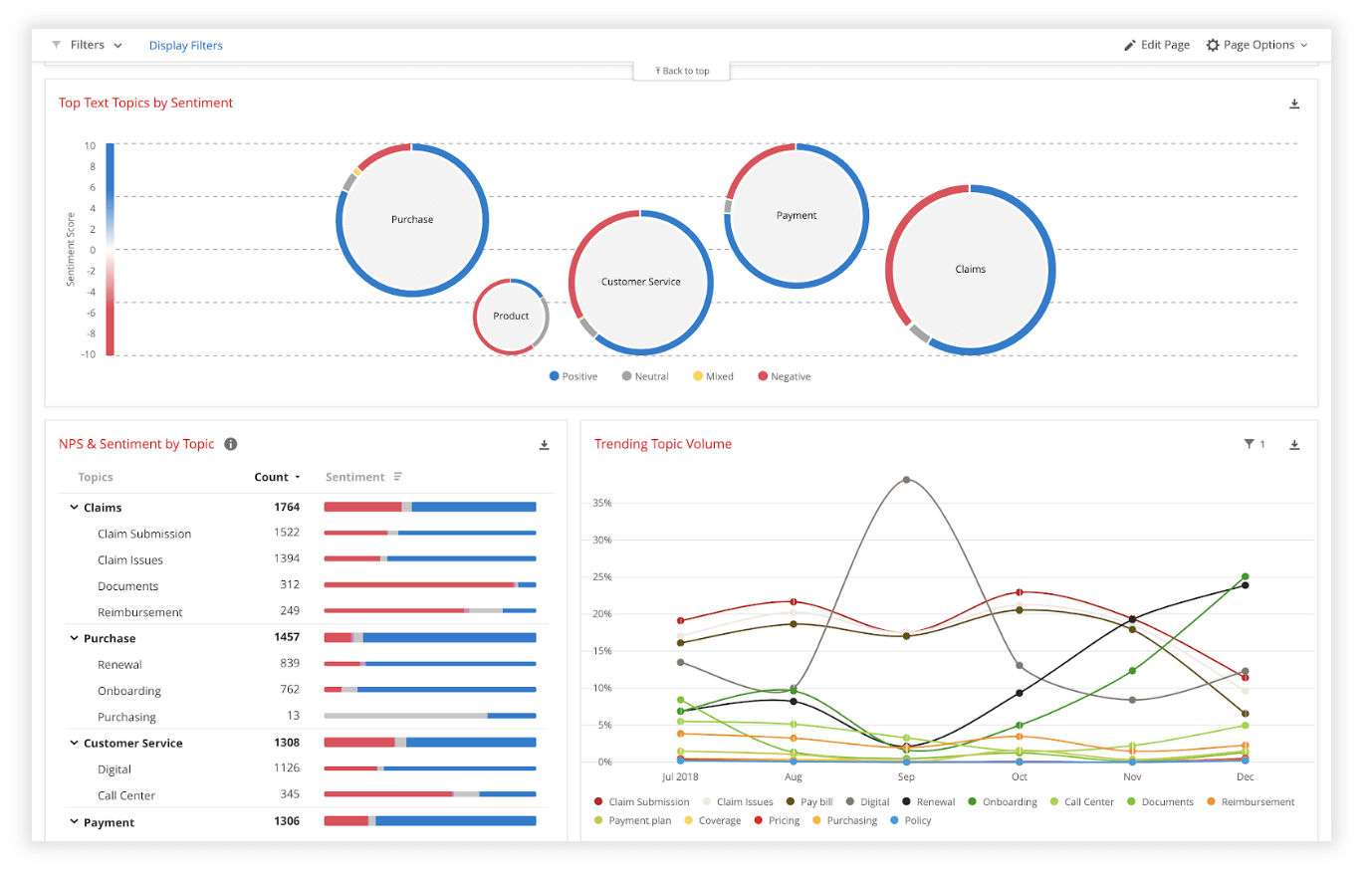
Data analysis
Qualitative interview data is unstructured, rich in content and difficult to analyze without the appropriate tools. Fortunately, machine learning and AI can once again make things faster and easier when you use qualitative methods like the research interview.
Text analysis tools and natural language processing software can ‘read’ your transcripts and voice data and identify patterns and trends across large volumes of text or speech. They can also perform khttps://www.qualtrics.com/experience-management/research/sentiment-analysis/
which assesses overall trends in opinion and provides an unbiased overall summary of how participants are feeling.
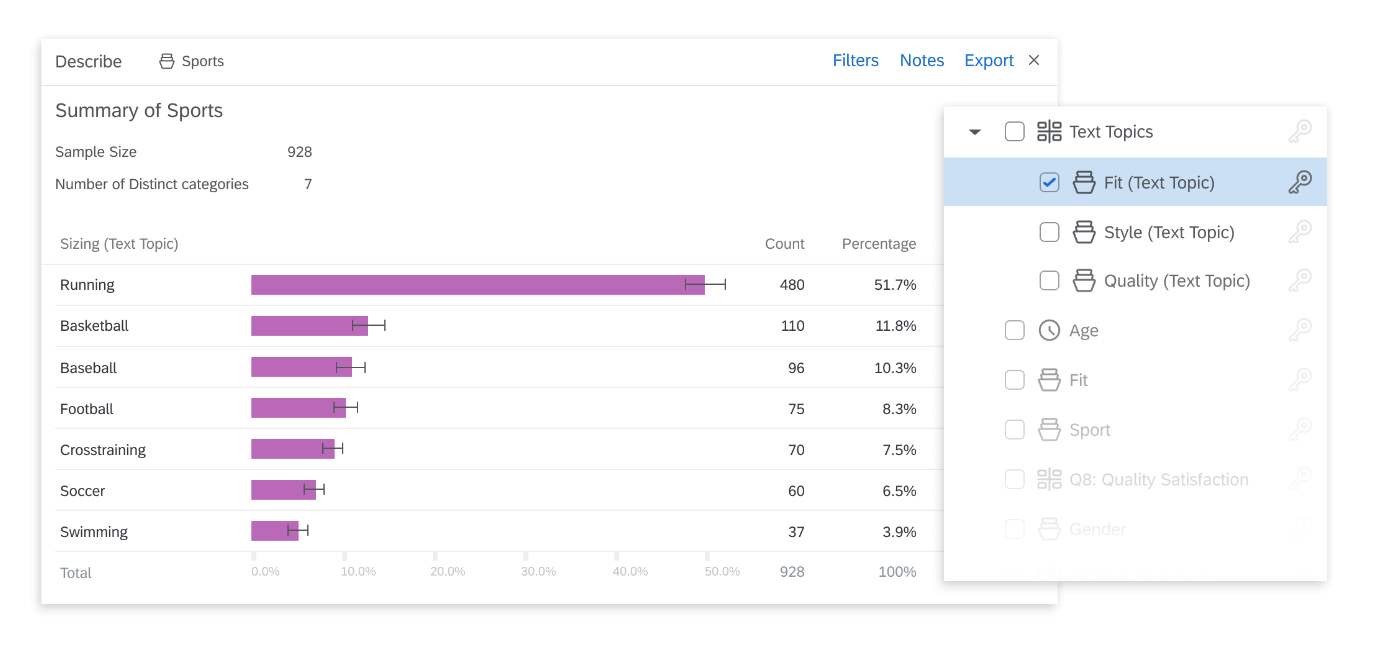
Another feature of text analysis tools is their ability to categorize information by topic, sorting it into groupings that help you organize your data according to the topic discussed.
All in all, interviews are a valuable technique for qualitative research in business, yielding rich and detailed unstructured data. Historically, they have only been limited by the human capacity to interpret and communicate results and conclusions, which demands considerable time and skill.
When you combine this data with AI tools that can interpret it quickly and automatically, it becomes easy to analyze and structure, dovetailing perfectly with your other business data. An additional benefit of natural language analysis tools is that they are free of subjective biases, and can replicate the same approach across as much data as you choose. By combining human research skills with machine analysis, qualitative research methods such as interviews are more valuable than ever to your business.
Related resources
Market intelligence 10 min read, marketing insights 11 min read, ethnographic research 11 min read, qualitative vs quantitative research 13 min read, qualitative research questions 11 min read, qualitative research design 12 min read, primary vs secondary research 14 min read, request demo.
Ready to learn more about Qualtrics?
Incorporating Interview Data
Introduction
When you incorporate original interview data into your writing, you are developing new ideas by using quotations and often sources that no one else has accessed. Drawing from interviews can liven up your writing, ground your big concepts within the specific circumstances of particular individuals, and introduce you to insights you might never have considered on your own. Additionally, interviews are an exciting way for you to provide a larger audience for people who might not otherwise have opportunities to share their stories, perceptions, and experiences.
There are lots of good reasons to incorporate original interview data into your writing. But doing so also involves making many, specific writing decisions. On this page we explore some of those decisions by considering: 1) the process by which interview data is gathered; 2) models for interview incorporation; and 3) identification of ways that writing with interview data can be like writing with information from any other source (as well as some of the unique writerly considerations that interviews raise).
Contents Before You Write Different Models of Incorporating Interview Data Summarizing, Paraphrasing, or Quoting Referring to your Interviewees Using Verbatim or Non-Verbatim
Before You Write
Of course, before you can incorporate interview data into your writing, you need to plan and conduct your interviews and begin to analyze your findings.
Interviewing is a common form of research and information gathering in many different fields and across many different genres. In order to develop and actualize a plan for why interviews will help you answer the questions you’re asking, whom you’ll interview, and what you’ll ask these subjects, you’ll want to consult a range of resources. Talk with your instructor, mentor, or advisor about common ways of approaching interviews for this assignment or in this discipline. Additionally, many undergraduate textbooks about research in the social sciences and humanities offer introductions to interviewing. We’ve listed a few great resources to help you learn more.
For comprehensive introductions to research methods used in the writing research that include some information about interviews, consider:
- Jackie Grutsch McKinney’s book Strategies for Writing Center Research —especially pages 55-69. While Grutsch McKinney’s is focused on writing center research, her close consideration of the different ways to structure interviews as well as how to plan and conduct them can be applied to all interview contexts. Additionally, her treatment of data analysis in chapter 8 provides a step-by-step guide for coding qualitative data—one of the approaches you might use to make sense of what your interview data means.
- Joyce Kinkead’s Researching Writing: An Introduction to Research Methods —especially pages 37-39. This is a potential textbook for that could be used for a class specifically about the formal study of writing. However, its direct and specific information about interviewing is applicable for any social science researcher preparing to use interviews for research.
These resources focus more specifically on qualitative research methods in particular and interviewing in particular:
- Robert Bogdan and Sari Knopp Biklen’s Qualitative Research for Education: An Introduction to Theories and Methods —especially pages 103-109. Bogdan and Knopp Biklen’s treatment of interview practices provides a brief overview of how to approach and implement this research methodology.
- Irving Seidman’s Interviewing as Qualitative Research: A Guide for Researchers in Education and the Social Sciences —especially pages 78-94. This entire book explores interview practices, logistics, and applications, but chapter six in particular usefully details particular interviewing techniques and provides transcripted examples of some of these strategic techniques in action.
The rest of the information on this page assumes that you have learned to develop and implement your interview plan, that you’ve analyzed the information you’ve gathered, and that you’re now ready to start weaving that information into your writing.
Different Models for Incorporating Interview Data
You can use interview data in many different ways. Most often, you will probably be making an argumentative or analytical point and illustrating and supporting it with evidence from your interviews. For example, in the following passage from the book Booty Capitalism: The Politics of Banking in the Philippines , Paul D. Hutchcroft, a political science professor at Australian National University, begins with an original claim, follows that with a quotation from an interview subject that exemplifies that claim, and then offers additional commentary on that issue. Note how the quotation from the interview both connects the concepts of banking and politics and introduces the prism metaphor that Hutchcroft continues into the next sentence.
The major focus of this [book] is two arenas that offer particular insights into the nature of relations between state and oligarchy in the banking system: bank supervision and selective credit allocation. “Banking,” observes one former bank president, “is a prism through which to understand power politics in the Philippines.” A study of the banking system highlights larger patterns at work within the political economy: how a predatory oligarchy extracts privilege from a patrimonial state, and how developmental policy objectives are continually choked out by a clamor of particularistic demands made by those who currently enjoy proximity to the political machinery. (7)
Generalizing about a Trend or Theme
Using information from an interview to support your claim is the primary purpose for incorporating interview data into your writing, but how you do this may change according to your specific intent. In what follows, we explore different models for weaving interview data into your writing and provide examples of what this looks like.
It is important to consider the politicization of the nationality responses in context. On the whole, the vast majority of republican executives did not try to influence the process, and the nationality question was a non-issue in the predominantly ethnically Russian regions. In my regional interviews I found that in the oblasts and krays, there were almost no reports of difficulty with the nationality question. Officials in those areas reported that respondents who were not ethnically Russian had no difficulty citing a different nationality. This finding corresponded with my observations of the enumeration process in Moscow. There were sporadic cases of respondents in ethnically mixed marriages registering one child as of one parent’s ethnic group and the other child as of the other parent’s ethnic group. However, this is a conceptual issue rather than a problem of politicization. ( 367-8 )
Quoting to Illustrate a Trend or Theme
Sometimes interviewees say things that are so strikingly similar that it is useful to draw attention to these complementary concepts and word choices by putting them together. In the following passage, Jane Calvert, a professor at the University of Edinburgh, and Joan Fujimura, a sociology professor at UW-Madison, use this strategy while writing about scientists’ responses to the new and developing field of systems biology. Note that these authors carefully tie quotations to specific anonymized interviewees through parenthetical citations.
In another US university, the decision to build an interdisciplinary research centre was top-down, initiated by university and funding administrators and initially opposed by most campus laboratory scientists. The building of new interdisciplinary structures is challenging for the existing disciplinary “fiefdoms” (Biologist19) and “silos” (Biologist9 and Biologist12) “where people feel protected and safe” (Biologist19) because they are not required to step outside of their “comfort zones” (Biologist7).
Putting Two Sources in Conversation with Each Other
Sometimes writers can use one interviewee to contribute to or complicate what another interviewee says. The following paragraph from Hutchcroft’s Booty Capitalism shows this practice at work. In addition to bringing two sources together, in this passage Hutchcroft also strategically incorporates paratextual insight gained from the interview process into his analysis. He uses the former governor’s laughter to showcase an attitude that directly contrasts with what the former bank supervisor says.
Even when the Central Bank has acted against those who milked their banks, former bank owners have been known to use personal connections, even up to the Supreme Court, to confound Central Bank discipline. Former Governor Jaime Laya noted that even martial law “didn’t seem to stop the lawsuits against Central Bank personnel.” He actually laughed as he told me how the Central Bank legal office has “never won a case.” But the former head of the bank supervision sector, who has herself been sued, doesn’t find it a laughing matter: “Why only in this country,” she exclaimed, “do the regulators go to the jail, and the bankers go scot-free?” (9)
Providing a Profile/Telling a Story
Sometimes your writing needs to focus on your interview subject as a full and complex individual. In order to analyze an issue, you need to write about this individual’s background, family, and previous experiences. In this situation, you’ll weave together information you gained from your interviews with quotations from this person. This kind of writing is common when you are using interviews to develop ethnographis case studies. In the following example of this technique, Kate Vieira, a professor in the Department of Curriculum and Instruction at UW-Madison, tells the story of Jocélia, an undocumented Brazilian immigrant living in Massachusetts:
Jocélia, a 22 year-old Brazilian woman who grew up in a favela (shanty town) in Brazil, came to the United States to study and to earn money. When her visa expired and the small sum she had borrowed from cousins ran out, she quit her ESL classes and began to work illegally. When I met her in 2008, she had been in the United States for 4 years, had managed to buy a house for her mother in Brazil, and had plans to buy another one for herself and a car. To earn money as an undocumented worker, she held down two jobs: one from 3 p.m. to midnight and another from 5 a.m. to afternoon. One evening, exhausted from having not slept in days, she nodded off as she drove home from work, resulting in a serious accident that led her to a friend’s house in South Mills and to a Catholic retreat. When I came here, I was not a youth who had fun. I only worked, and this made me a little frustrated, you know? Sad, lonely, understand? And nobody could change my mind. I had to work . . . But the Lord showed me something different, that I can’t live only for work . . . So I went there [to the retreat] and I really felt that the Lord touched us. It was a very good experience . . . (444)
Attending to Language
As explored in greater depth in the discussion about verbatim transcription , sometimes you want to analyze or consider the language an individual uses or the implications of certain kinds of words or even pauses. For example, in the following passage, Beth Godbee, a writing and rhetoric professor at Marquette University, meticulously considers the implications of her subjects’ specific words and phrasing. Although this example is taken from Godbee’s analysis of a conversation she recorded between a writer Susan and a writing center tutor Kim as opposed to a direct interview she conducted, the attention she pays to language could just as well be applied to information from an interview.
Kim reinforces Susan’s qualifications: “You’re gonna—you’re the specialist in this area. You know these kids; you see what know the effects are, and maybe where some change could be made” (lines 558-561). Here Kim revises her projection of Susan as a “specialist” in the future tense (“gonna,” as in “you’re going to be”) to a statement of her current position (“you’re,” or “you are now”). By repairing her speech mid-utterance, Kim emphasizes Susan’s current status and qualifications to write, thereby reframing her institutional power to assert her right to speak. (185)
Summarizing, Paraphrasing, or Quoting
As the above examples show, interview data is incorporated into writing through summaries, paraphrases, or quotations. In some ways this makes working with interviews just like working from any other kind of outside. As you choose between summarizing, paraphrasing, or quoting, a guiding question for you to consider is: What is most important about this information?
- Is it the overall story it tells or the general perspective it provides? Then summarizing might be the best option.
- Is it the particular take on a complex issue? Then paraphrasing that idea in your own words to make it as understandable as possible might be best.
- Is it the memorability, specificity, or authenticity of the language the source used? Then probably go with a quote, but be sure to contextualize this quotation by providing necessary background and commentary.
Of course, in working with interview data, you might go with all three incorporation strategies by, for example, summarizing early in a paragraph to provide an overall sense of what this source is saying, paraphrasing a key idea or two, and then including a poignant quotation that exemplifies the argument you are making. For more information about quoting and paraphrasing outside sources in your writing, check out our resources on this issue .
Referring to your Interviewees
In certain writing situations, you are expected to identify the people you interviewed by using their real names. This is often the case in journalistic writing as well as when you have consulted with an expert on an issue. But, even in these writing contexts, you must receive permission from them to associate their words and insights with their names by clearly establishing whether or not they are talking with you “on the record.”
However, when you are conducting interviews for academic research, you are frequently expected to use pseudonyms so that your subjects’ responses are confidential. Protecting your subjects’ privacy should be your primary priority. They are giving you access to personal experiences and trusting you with their individual insights and observations; you must honor that trust by anonymizing their identities so that readers can’t figure out who your subjects were. Developing a research methodology that keeps all of your data confidential is an important part of the IRB (Internal Review Board) process, and in order to receive permission to do research at your institution you’ll need a plan that outlines how you’ll achieve confidentiality. Part of that plan will involve using different names for your subjects. But selecting pseudonyms is a bigger issue than just choosing different names at random.
Ruth Allen and Janine L. Wiles, Social and Community Health scholars at the University of Auckland, have closely considered the many issues surrounding pseudonym selection in connection to their original psychological and health-related research. They advocate that researchers think critically about this process and even bring their subjects into these discussions of identity and confidentiality. You need to be thoughtful about what aspects of your subjects’ true identities you are communicating or obscuring through the pseudonyms you use. The following questions are adapted from ones Allen and Wiles recommend researchers ask themselves when preparing to use pseudonyms for participants:
- Does the researcher or the participant choose the pseudonym? How does this issue get talked about with the participants?
- Is it important, valuable, or expected to use first name or also include last names and/or titles (i.e., Cara, Mr. Terrance, Dr. Jean Nichols)?
- Within the context of this writing, should the names to be associated with a specific gender, ethnicity, and/or culture? Should those nominal identity markers align with the participants’ actual identities?
- Do pseudonyms need to be selected for other people, places, activities, and organizations mentioned in the interview? And if so, who makes those choices?
How you answer these questions should be informed by your specific context. For example, in relation to that fourth question, if a participant is talking supportively about a small on-campus organization that you want to bring attention to through your writing, it might make sense to refer to this organization by name even though its size might make it harder to disguise your participant’s identity. However, if your interviewee is speaking critically about a large, multi-national corporation where she works, you might want to develop a pseudonym for that company in order to protect this individual as much as possible.
Using Verbatim or Non-Verbatim
When you are conducting interviews, you are engaging people in very focused conversation. But when we converse, we say “like” a lot and “um” and “ah.” We start sentences and then interrupt ourselves and never return to complete those earlier thoughts. Conversation is never as direct and naturally coherent as writing can be. As a result, when you’re representing other people’s speech, you need to decide if you’ll be employing what is called “verbatim transcription” or “non-verbatim transcription.”
In “verbatim transcriptions,” you write out what people say exactly as they say it. You include all the filler words, false starts, and grammatical inconsistencies. You may even choose to include coughs and laughs. Scholars have traditionally upheld verbatim accounts as being accurate depictions of the interview process, but as Blake Poland pointed out, “much of the emotional context of the interview as well as nonverbal communication are not captured at all well in audiotape records, so that the audiotape itself is not strictly a verbatim record of the interview” (291). “Non-verbatim transcriptions,” (sometimes called “intelligent transcription”) respond to this acknowledged gap between the complexities of real conversation and the limitations of writing by encouraging writers to focus on the primary substance of participants’ quotes. In “non-verbatim transcriptions, you eliminate the unnecessary utterances like “er,” “well,” and “you know” and just include the foundational meaning of the interviewees’ words.” For example:
Verbatim Transcription : Well, you see, I was [pause] the problem, as I saw it, was more of a, a matter of representation, you know? How can I, like, be the one that’s just out there just declaring the way things are when I’ve not even, like, you know, experiencing the whole process for myself? Non-verbatim Transcription : The problem, as I saw it, was more a matter of representation. How can I be the one that’s out there declaring the way things are when I’ve not even experienced the whole process for myself?
The choice to use verbatim or non-verbatim transcription in quoting your participants should be informed by intentional considerations you are making as a writer. There are good reasons to use either forms. As Mahesh Kumar has identified in a blog post for the Transcription Certification Institute, verbatim transcription is useful for showcasing the thought process by which interview participants develop their ideas. False starts and self-corrections track down how someone is thinking about an issue in real time, and some fillers can be useful expressions of personality. Additionally, some linguistics research and conversation analysis methodologies expect highly structured, verbatim transcriptions that even account for pauses and simultaneous dialogue. However, quotations presented through non-verbatim transcriptions are clearer and easier to read and enable you to present your interview subjects as articulate (Poland 292). Whether you go with verbatim or non-verbatim transcription, make sure that you are being consistent with this choice across your article, paper, report, or essay. Also, if it’s common in the genre you are writing to discuss your methodology choices, it may be useful to clarify which transcription form you have chosen to use and why this was an appropriate choice.
Works Cited
Allen, Ruth E.S., and Janine L. Wiles. “A Rose by Any Other Name: Participants Choosing Research Pseudonyms.” Qualitative Research in Psychology , Dec. 2015. Research Gate , doi: 10.1080/14780887.2015.1133746.
Bogdan, Robert C., and Sari Knopp Biklen. Qualitative Research for Education: An Introduction to Theories and Methods . 5 th ed., Pearson, 2007.
Calvert, Jane, and Joan H. Fujimura. “Calculating Life? Duelling Discourses in Interdisciplinary Systems Biology.” Studies in History and Philosophy of Science Part C: Studies in History and Philosophy of Biological and Biomedical Sciences , vol. 42, no. 2l, 2011. Science Direct , https://doi.org/10.1016/j.shpsc.2010.11.022 .
Godbee, Beth. “Toward Explaining the Transformative Power of Talk About, Around, and for Writing.” Research in the Teaching of English , vol. 47, no. 2, 2012, pp. 171-97.
Grutsch McKinney, Jackie. Strategies for Writing Center Research . Parlor Press, 2016.
Herrera, Yoshiko M. “The 2002 Russian Census: Institutional Reform at Goskomstar.” Post-Soviet Affairs , vol, 20, no. 4, 2004, pp. 350-86.
Hutchcroft, Paul D. Booty Capitalism: The Politics of Banking in the Philippines , Ateneo de Manila University Press, 1998.
Kinkead, Joyce. Researching Writing: An Introduction to Research Methods . University Press of Colorado, 2015.
Kumar, Mahesh. “Verbatim Vs Non-Verbatim Transcription: Differences, Requirements, & Jobs.” Transcription Certification Institute , 5 December 2017. Accessed online 19 June 2017. https://blog.transcriptioncertificationinstitute.org/verbatim-vs-non-verbatim-transcription-differences-requirements-jobs/.
Poland, Blake D. “Transcription Quality as an Aspect of Rigor in Qualitative Research.” Qualitative Inquiry , no. 1, vol. 3, 1995, pp. 290-310.
Seidman, Irving. Interviewing as Qualitative Research: A Guide for Researchers in Education and the Social Sciences . 3 rd ed., Teachers College Press, 2006.
Vieira, Kate. “Undocumented in a Documentary Society: Textual Borders and Transnational Religious Literacies.” Written Communication , vol 28, no. 4, 2011, pp. 436-61.

Academic and Professional Writing
This is an accordion element with a series of buttons that open and close related content panels.
Analysis Papers
Reading Poetry
A Short Guide to Close Reading for Literary Analysis
Using Literary Quotations
Play Reviews
Writing a Rhetorical Précis to Analyze Nonfiction Texts
Grant Proposals
Planning and Writing a Grant Proposal: The Basics
Additional Resources for Grants and Proposal Writing
Job Materials and Application Essays
Writing Personal Statements for Ph.D. Programs
- Before you begin: useful tips for writing your essay
- Guided brainstorming exercises
- Get more help with your essay
- Frequently Asked Questions
Resume Writing Tips
CV Writing Tips
Cover Letters
Business Letters
Proposals and Dissertations
Resources for Proposal Writers
Resources for Dissertators
Research Papers
Planning and Writing Research Papers
Quoting and Paraphrasing
Writing Annotated Bibliographies
Creating Poster Presentations
Writing an Abstract for Your Research Paper
Thank-You Notes
Advice for Students Writing Thank-You Notes to Donors
Reading for a Review
Critical Reviews
Writing a Review of Literature
Scientific Reports
Scientific Report Format
Sample Lab Assignment
Writing for the Web
Writing an Effective Blog Post
Writing for Social Media: A Guide for Academics

- Learn How to Use the Library
- Providers & Employees
- Research Help
- All Research Guides
Conducting Research Interviews
The interviewer mindset, quick tips for preparing, developing questions.
- Conducting the Interview
- Applying & Using the Interview
While the research interview is a one-on-one interaction, it's not a normal conversation. As the interviewer, it's expected that you:
- Are knowledgeable on the topic of the interview (this may require some background research)
- Are able to structure and guide the interview to keep it relevant but flexible
- Are able to remember and interpret the information gained in the interview
- Are sensitive to the interviewee's position and their rights
- Do preliminary research on the topic and the interviewee so that you enter the interview with an understanding of what will be discussed.
- Reflect on your goals. What should the interview accomplish? What is important to have recorded in the interview, and why is it important? How can you make the process easy for the interviewee?
- Create a list of topics and questions to explore during the interview. This should not be a strict checklist or a script; rather, it should function as a guide to ensure that you cover all of the content and that the interview stays focused.
- Create an open line of dialog with your interviewee before the interview so that you are comfortable with each other. This can involve going over the process, offering to answer any of their questions, verifying your time and place for the interview, etc.
- Choose and thoroughly familiarize yourself with your recording equipment to minimize any potential issues that may arise during the actual interview.
- Choose an interview space that is relaxed, comfortable, and quiet. You are having a conversation with your interviewee, not an interrogation.
- If you have never interviewed before, feel free to practice for the interview with friends, family, or peers. This will make sure you are prepared for the real thing.
Characteristics of good interview questions
- Open-ended and elicit a long response from the interviewee (can't be answered yes/no or with one word)
- Focus on the experience of the interviewee
- Don't lead the interviewee toward a particular response
- Address a single issue/point (i.e. don't ask multi-part questions)
Writing interview questions
Harvard's Department of Sociology provides some steps to help guide you in the process of writing interview questions (see the link to the guide below).
- Write down the larger research questions of the study. Outline the broad areas of knowledge that are relevant to answering these questions.
- Develop questions within each of these major areas, shaping them to fit particular kinds of respondents. The goal here is to tap into their experiences and expertise.
- Adjust the language of the interview according to the respondent (child, professional, etc.).
- Take care to word questions so that respondents are motivated to answer as completely and honestly as possible.
- Ask “how” questions rather than “why” questions to get stories of process rather than acceptable “accounts” of behavior. “How did you come to join this group . . .?”
- Develop probes that will elicit more detailed and elaborate responses to key questions. The more detail, the better!
- Begin the interview with a “warm-up” question—something that the respondent can answer easily and at some length (though not too long). It doesn’t have to pertain directly to what you are trying to find out (although it might), but this initial rapport-building will put you more at ease with one another and thus will make the rest of the interview flow more smoothly.
- Think about the logical flow of the interview. What topics should come first? What follows more or less “naturally”? This may take some adjustment after several interviews.
- Difficult or potentially embarrassing questions should be asked toward the end of the interview, when rapport has been established.
- The last question should provide some closure for the interview, and leave the respondent feeling empowered, listened to, or otherwise glad that they talked to you.
- Strategies for Qualitative Interviews This handy guide from Harvard's Department of Sociology provides guidance on getting into the interviewer mindset as well as developing and writing interview questions.
Depending on the nature of your assignment or research, you may or may not need to record and transcribe the interview. Review the pros and cons to determine whether recording and transcribing will be worthwhile for you.
- Helps you to recall more details of the interview
- Helps you to thoroughly examine the interview
- It allows other researchers to interpret and reuse the data in new ways
- May be off-putting to interviewees or make them feel pressured
- Transcribing is a time-consuming process; even using a transcription software requires a detailed review of the text
"Strategies for Qualitative Interviews" (n.d.) Harvard. See link above..
- << Previous: Home
- Next: Conducting the Interview >>
- Last Updated: Mar 25, 2024 8:55 AM
- URL: https://aultman.libguides.com/interviews
Aultman Health Sciences Library
Aultman Education Center, C2-230, 2600 Sixth St SW, Canton, OH 44710 | 330-363-5000 | [email protected]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Basic Clin Pharm
- v.5(4); September 2014-November 2014
Qualitative research method-interviewing and observation
Shazia jamshed.
Department of Pharmacy Practice, Kulliyyah of Pharmacy, International Islamic University Malaysia, Kuantan Campus, Pahang, Malaysia
Buckley and Chiang define research methodology as “a strategy or architectural design by which the researcher maps out an approach to problem-finding or problem-solving.”[ 1 ] According to Crotty, research methodology is a comprehensive strategy ‘that silhouettes our choice and use of specific methods relating them to the anticipated outcomes,[ 2 ] but the choice of research methodology is based upon the type and features of the research problem.[ 3 ] According to Johnson et al . mixed method research is “a class of research where the researcher mixes or combines quantitative and qualitative research techniques, methods, approaches, theories and or language into a single study.[ 4 ] In order to have diverse opinions and views, qualitative findings need to be supplemented with quantitative results.[ 5 ] Therefore, these research methodologies are considered to be complementary to each other rather than incompatible to each other.[ 6 ]
Qualitative research methodology is considered to be suitable when the researcher or the investigator either investigates new field of study or intends to ascertain and theorize prominent issues.[ 6 , 7 ] There are many qualitative methods which are developed to have an in depth and extensive understanding of the issues by means of their textual interpretation and the most common types are interviewing and observation.[ 7 ]
Interviewing
This is the most common format of data collection in qualitative research. According to Oakley, qualitative interview is a type of framework in which the practices and standards be not only recorded, but also achieved, challenged and as well as reinforced.[ 8 ] As no research interview lacks structure[ 9 ] most of the qualitative research interviews are either semi-structured, lightly structured or in-depth.[ 9 ] Unstructured interviews are generally suggested in conducting long-term field work and allow respondents to let them express in their own ways and pace, with minimal hold on respondents’ responses.[ 10 ]
Pioneers of ethnography developed the use of unstructured interviews with local key informants that is., by collecting the data through observation and record field notes as well as to involve themselves with study participants. To be precise, unstructured interview resembles a conversation more than an interview and is always thought to be a “controlled conversation,” which is skewed towards the interests of the interviewer.[ 11 ] Non-directive interviews, form of unstructured interviews are aimed to gather in-depth information and usually do not have pre-planned set of questions.[ 11 ] Another type of the unstructured interview is the focused interview in which the interviewer is well aware of the respondent and in times of deviating away from the main issue the interviewer generally refocuses the respondent towards key subject.[ 11 ] Another type of the unstructured interview is an informal, conversational interview, based on unplanned set of questions that are generated instantaneously during the interview.[ 11 ]
In contrast, semi-structured interviews are those in-depth interviews where the respondents have to answer preset open-ended questions and thus are widely employed by different healthcare professionals in their research. Semi-structured, in-depth interviews are utilized extensively as interviewing format possibly with an individual or sometimes even with a group.[ 6 ] These types of interviews are conducted once only, with an individual or with a group and generally cover the duration of 30 min to more than an hour.[ 12 ] Semi-structured interviews are based on semi-structured interview guide, which is a schematic presentation of questions or topics and need to be explored by the interviewer.[ 12 ] To achieve optimum use of interview time, interview guides serve the useful purpose of exploring many respondents more systematically and comprehensively as well as to keep the interview focused on the desired line of action.[ 12 ] The questions in the interview guide comprise of the core question and many associated questions related to the central question, which in turn, improve further through pilot testing of the interview guide.[ 7 ] In order to have the interview data captured more effectively, recording of the interviews is considered an appropriate choice but sometimes a matter of controversy among the researcher and the respondent. Hand written notes during the interview are relatively unreliable, and the researcher might miss some key points. The recording of the interview makes it easier for the researcher to focus on the interview content and the verbal prompts and thus enables the transcriptionist to generate “verbatim transcript” of the interview.
Similarly, in focus groups, invited groups of people are interviewed in a discussion setting in the presence of the session moderator and generally these discussions last for 90 min.[ 7 ] Like every research technique having its own merits and demerits, group discussions have some intrinsic worth of expressing the opinions openly by the participants. On the contrary in these types of discussion settings, limited issues can be focused, and this may lead to the generation of fewer initiatives and suggestions about research topic.
Observation
Observation is a type of qualitative research method which not only included participant's observation, but also covered ethnography and research work in the field. In the observational research design, multiple study sites are involved. Observational data can be integrated as auxiliary or confirmatory research.[ 11 ]
Research can be visualized and perceived as painstaking methodical efforts to examine, investigate as well as restructure the realities, theories and applications. Research methods reflect the approach to tackling the research problem. Depending upon the need, research method could be either an amalgam of both qualitative and quantitative or qualitative or quantitative independently. By adopting qualitative methodology, a prospective researcher is going to fine-tune the pre-conceived notions as well as extrapolate the thought process, analyzing and estimating the issues from an in-depth perspective. This could be carried out by one-to-one interviews or as issue-directed discussions. Observational methods are, sometimes, supplemental means for corroborating research findings.
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
9.2 Qualitative interviews
Learning objectives.
- Define interviews from the social scientific perspective
- Identify when it is appropriate to employ interviews as a data-collection strategy
- Identify the primary aim of in-depth interviews
- Describe what makes qualitative interview techniques unique
- Define the term interview guide and describe how to construct an interview guide
- Outline the guidelines for constructing good qualitative interview questions
- Describe how writing field notes and journaling function in qualitative research
- Identify the strengths and weaknesses of interviews
Knowing how to create and conduct a good interview is an essential skill. Interviews are used by market researchers to learn how to sell their products, and journalists use interviews to get information from a whole host of people from VIPs to random people on the street. Police use interviews to investigate crimes.

In social science, interviews are a method of data collection that involves two or more people exchanging information through a series of questions and answers. The questions are designed by the researcher to elicit information from interview participants on a specific topic or set of topics. These topics are informed by the research questions. Typically, interviews involve an in-person meeting between two people—an interviewer and an interviewee — but interviews need not be limited to two people, nor must they occur in-person.
The question of when to conduct an interview might be on your mind. Interviews are an excellent way to gather detailed information. They also have an advantage over surveys—they can change as you learn more information. In a survey, you cannot change what questions you ask if a participant’s response sparks some follow-up question in your mind. All participants must get the same questions. The questions you decided to put on your survey during the design stage determine what data you get. In an interview, however, you can follow up on new and unexpected topics that emerge during the conversation. Trusting in emergence and learning from participants are hallmarks of qualitative research. In this way, interviews are a useful method to use when you want to know the story behind the responses you might receive in a written survey.
Interviews are also useful when the topic you are studying is rather complex, requires lengthy explanation, or needs a dialogue between two people to thoroughly investigate. Also, if people will describe the process by which a phenomenon occurs, like how a person makes a decision, then interviews may be the best method for you. For example, you could use interviews to gather data about how people reach the decision not to have children and how others in their lives have responded to that decision. To understand these “how’s” you would need to have some back-and-forth dialogue with respondents. When they begin to tell you their story, inevitably new questions that hadn’t occurred to you from prior interviews would come up because each person’s story is unique. Also, because the process of choosing not to have children is complex for many people, describing that process by responding to closed-ended questions on a survey wouldn’t work particularly well.
Interview research is especially useful when:
- You wish to gather very detailed information
- You anticipate wanting to ask respondents follow-up questions based on their responses
- You plan to ask questions that require lengthy explanation
- You are studying a complex or potentially confusing topic to respondents
- You are studying processes, such as how people make decisions
Qualitative interviews are sometimes called intensive or in-depth interviews. These interviews are semi-structured ; the researcher has a particular topic about which she would like to hear from the respondent, but questions are open-ended and may not be asked in exactly the same way or in exactly the same order to each and every respondent. For in-depth interviews , the primary aim is to hear from respondents about what they think is important about the topic at hand and to hear it in their own words. In this section, we’ll take a look at how to conduct qualitative interviews, analyze interview data, and identify some of the strengths and weaknesses of this method.
Constructing an interview guide
Qualitative interviews might feel more like a conversation than an interview to respondents, but the researcher is in fact usually guiding the conversation with the goal in mind of gathering specific information from a respondent. Qualitative interviews use open-ended questions, which are questions that a researcher poses but does not provide answer options for. Open-ended questions are more demanding of participants than closed-ended questions because they require participants to come up with their own words, phrases, or sentences to respond.
In a qualitative interview, the researcher usually develops an interview guide in advance to refer to during the interview (or memorizes in advance of the interview). An interview guide is a list of questions or topics that the interviewer hopes to cover during the course of an interview. It is called a guide because it is simply that—it is used to guide the interviewer, but it is not set in stone. Think of an interview guide like an agenda for the day or a to-do list—both probably contain all the items you hope to check off or accomplish, though it probably won’t be the end of the world if you don’t accomplish everything on the list or if you don’t accomplish it in the exact order that you have it written down. Perhaps new events will come up that cause you to rearrange your schedule just a bit, or perhaps you simply won’t get to everything on the list.
Interview guides should outline issues that a researcher feels are likely to be important. Because participants are asked to provide answers in their own words and to raise points they believe are important, each interview is likely to flow a little differently. While the opening question in an in-depth interview may be the same across all interviews, from that point on, what the participant says will shape how the interview proceeds. Sometimes participants answer a question on the interview guide before it is asked. When the interviewer comes to that question later on in the interview, it’s a good idea to acknowledge that they already addressed part of this question and ask them if they have anything to add to their response. All of this uncertainty can make in-depth interviewing exciting and rather challenging. It takes a skilled interviewer to be able to ask questions; listen to respondents; and pick up on cues about when to follow up, when to move on, and when to simply let the participant speak without guidance or interruption.
As we’ve discussed, interview guides can list topics or questions. The specific format of an interview guide might depend on your style, experience, and comfort level as an interviewer or with your topic. Figure 9.1 provides an example of an interview guide for a study of how young people experience workplace sexual harassment. The guide is topic-based, rather than a list of specific questions. The ordering of the topics is important, though how each comes up during the interview may vary.

For interview guides that use questions, there can also be specific words or phrases for follow-up in case the participant does not mention those topics in their responses. These probes , as well as the questions are written out in the interview guide, but may not always be used. Figure 9.2 provides an example of an interview guide that uses questions rather than topics.

As you might have guessed, interview guides do not appear out of thin air. They are the result of thoughtful and careful work on the part of a researcher. As you can see in both of the preceding guides, the topics and questions have been organized thematically and in the order in which they are likely to proceed (though keep in mind that the flow of a qualitative interview is in part determined by what a respondent has to say). Sometimes qualitative interviewers may create two versions of the interview guide: one version contains a very brief outline of the interview, perhaps with just topic headings, and another version contains detailed questions underneath each topic heading. In this case, the researcher might use the very detailed guide to prepare and practice in advance of actually conducting interviews and then just bring the brief outline to the interview. Bringing an outline, as opposed to a very long list of detailed questions, to an interview encourages the researcher to actually listen to what a participant is saying. An overly detailed interview guide can be difficult to navigate during an interview and could give respondents the mis-impression the interviewer is more interested in the questions than in the participant’s answers.
Constructing an interview guide often begins with brainstorming. There are no rules at the brainstorming stage—simply list all the topics and questions that come to mind when you think about your research question. Once you’ve got a pretty good list, you can begin to pare it down by cutting questions and topics that seem redundant and group similar questions and topics together. If you haven’t done so yet, you may also want to come up with question and topic headings for your grouped categories. You should also consult the scholarly literature to find out what kinds of questions other interviewers have asked in studies of similar topics and what theory indicates might be important. As with quantitative survey research, it is best not to place very sensitive or potentially controversial questions at the very beginning of your qualitative interview guide. You need to give participants the opportunity to warm up to the interview and to feel comfortable talking with you. Finally, get some feedback on your interview guide. Ask your friends, other researchers, and your professors for some guidance and suggestions once you’ve come up with what you think is a strong guide. Chances are they’ll catch a few things you hadn’t noticed. Once you begin your interviews, your participants may also suggest revisions or improvements.
In terms of the specific questions you include in your guide, there are a few guidelines worth noting. First, avoid questions that can be answered with a simple yes or no. Try to rephrase your questions in a way that invites longer responses from your interviewees. If you choose to include yes or no questions, be sure to include follow-up questions. Remember, one of the benefits of qualitative interviews is that you can ask participants for more information—be sure to do so. While it is a good idea to ask follow-up questions, try to avoid asking “why” as your follow-up question, as this particular question can come off as confrontational, even if that is not your intent. Often people won’t know how to respond to “why,” perhaps because they don’t even know why themselves. Instead of asking “why,” you say something like, “Could you tell me a little more about that?” This allows participants to explain themselves further without feeling that they’re being doubted or questioned in a hostile way.
Also, try to avoid phrasing your questions in a leading way. For example, rather than asking, “Don’t you think most people who don’t want to have children are selfish?” you could ask, “What comes to mind for you when you hear someone doesn’t want to have children?” Finally, remember to keep most, if not all, of your questions open-ended. The key to a successful qualitative interview is giving participants the opportunity to share information in their own words and in their own way. Documenting the decisions made along the way regarding which questions are used, thrown out, or revised can help a researcher remember the thought process behind the interview guide when she is analyzing the data. Additionally, it promotes the rigor of the qualitative project as a whole, ensuring the researcher is proceeding in a reflective and deliberate manner that can be checked by others reviewing her study.
Recording qualitative data
Even after the interview guide is constructed, the interviewer is not yet ready to begin conducting interviews. The researcher has to decide how to collect and maintain the information that is provided by participants. Researchers keep field notes or written recordings produced by the researcher during the data collection process. Field notes can be taken before, during, or after interviews. Field notes help researchers document what they observe, and in so doing, they form the first step of data analysis. Field notes may contain many things—observations of body language or environment, reflections on whether interview questions are working well, and connections between ideas that participants share.

Unfortunately, even the most diligent researcher cannot write down everything that is seen or heard during an interview. In particular, it is difficult for a researcher to be truly present and observant if she is also writing down everything the participant is saying. For this reason, it is quite common for interviewers to create audio recordings of the interviews they conduct. Recording interviews allows the researcher to focus on the interaction with the interview participant.
Of course, not all participants will feel comfortable being recorded and sometimes even the interviewer may feel that the subject is so sensitive that recording would be inappropriate. If this is the case, it is up to the researcher to balance excellent note-taking with exceptional question-asking and even better listening.
Whether you will be recording your interviews or not (and especially if not), practicing the interview in advance is crucial. Ideally, you’ll find a friend or two willing to participate in a couple of trial runs with you. Even better, find a friend or two who are similar in at least some ways to your sample. They can give you the best feedback on your questions and your interview demeanor.
Another issue interviewers face is documenting the decisions made during the data collection process. Qualitative research is open to new ideas that emerge through the data collection process. For example, a participant might suggest a new concept you hadn’t thought of before or define a concept in a new way. This may lead you to create new questions or ask questions in a different way to future participants. These processes should be documented in a process called journaling or memoing. Journal entries are notes to yourself about reflections or methodological decisions that emerge during the data collection process. Documenting these are important, as you’d be surprised how quickly you can forget what happened. Journaling makes sure that when it comes time to analyze your data, you remember how, when, and why certain changes were made. The discipline of journaling in qualitative research helps to ensure the rigor of the research process—that is its trustworthiness and authenticity which we will discuss later in this chapter.
Strengths and weaknesses of qualitative interviews
As we’ve mentioned in this section, qualitative interviews are an excellent way to gather detailed information. Any topic can be explored in much more depth with interviews than with almost any other method. Not only are participants given the opportunity to elaborate in a way that is not possible with other methods such as survey research, but they also are able share information with researchers in their own words and from their own perspectives. Whereas, quantitative research asks participants to fit their perspectives into the limited response options provided by the researcher. And because qualitative interviews are designed to elicit detailed information, they are especially useful when a researcher’s aim is to study social processes or the “how” of various phenomena. Yet another, and sometimes overlooked, benefit of in-person qualitative interviews is that researchers can make observations beyond those that a respondent is orally reporting. A respondent’s body language, and even their choice of time and location for the interview, might provide a researcher with useful data.
Of course, all these benefits come with some drawbacks. As with quantitative survey research, qualitative interviews rely on respondents’ ability to accurately and honestly recall specific details about their lives, circumstances, thoughts, opinions, or behaviors. Further, as you may have already guessed, qualitative interviewing is time-intensive and can be quite expensive. Creating an interview guide, identifying a sample, and conducting interviews are just the beginning. Writing out what was said in interviews and analyzing the qualitative interview data are time consuming processes. Keep in mind you are also asking for more of participants’ time than if you’d simply mailed them a questionnaire containing closed-ended questions. Conducting qualitative interviews is not only labor-intensive but can also be emotionally taxing. Seeing and hearing the impact that social problems have on respondents is difficult. Researchers embarking on a qualitative interview project should keep in mind their own abilities to receive stories that may be difficult to hear.
Key Takeaways
- Understanding how to design and conduct interview research is a useful skill to have.
- In a social scientific interview, two or more people exchange information through a series of questions and answers.
- Interview research is often used when detailed information is required and when a researcher wishes to examine processes.
- In-depth interviews are semi-structured interviews where the researcher has topics and questions in mind to ask, but questions are open-ended and flow according to how the participant responds to each.
- Interview guides can vary in format but should contain some outline of the topics you hope to cover during the course of an interview.
- Qualitative interviews allow respondents to share information in their own words and are useful for gathering detailed information and understanding social processes.
- Field notes and journaling are ways to document thoughts and decisions about the research process
- Drawbacks of qualitative interviews include reliance on respondents’ accuracy and their intensity in terms of time, expense, and possible emotional strain.
- Field notes- written notes produced by the researcher during the data collection process
- In-depth interviews- interviews in which researchers hear from respondents about what they think is important about the topic at hand in the respondent’s own words
- Interviews- a method of data collection that involves two or more people exchanging information through a series of questions and answers
- Interview guide- a list of questions or topics that the interviewer hopes to cover during the course of an interview
- Journaling- making notes of emerging issues and changes during the research process
- Semi-structured interviews- questions are open ended and may not be asked in exactly the same way or in exactly the same order to each and every respondent
Image attributions
interview restaurant a pair by alda2 CC-0
questions by geralt CC-0
Figure 9.1 is copied from Blackstone, A. (2012) Principles of sociological inquiry: Qualitative and quantitative methods. Saylor Foundation. Retrieved from: https://saylordotorg.github.io/text_principles-of-sociological-inquiry-qualitative-and-quantitative-methods/ Shared under CC-BY-NC-SA 3.0 License
writing by StockSnap CC-0
Foundations of Social Work Research Copyright © 2020 by Rebecca L. Mauldin is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License , except where otherwise noted.
Share This Book
Qualitative Interview Questions: Guidance for Novice Researchers
- September 2020
- The Qualitative Report
- This person is not on ResearchGate, or hasn't claimed this research yet.
Discover the world's research
- 25+ million members
- 160+ million publication pages
- 2.3+ billion citations

- Betül ERSOY
- D Alkhodary
- M Alnawaiseh
- Ahmad B Ahmad
- Mark Holton

- Jennifer Yphantides
- Iman Setia Harefa

- Eleni Gesch-Karamanlidis
- Steinar Kvale
- Julie Bettie
- Barney G. Glaser
- Anselm L. Strauss
- A. I. Richards

- Barbara Snell Dohrenwend
- David Klein
- Y.S. Lincoln
- John W. Creswell
- David S. Cordray
- Michael Quinn Patton
- M.Q. Patton
- Recruit researchers
- Join for free
- Login Email Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google Welcome back! Please log in. Email · Hint Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google No account? Sign up
- Advanced search
Advanced Search
Discourses of Distrust: How Lack of Trust in the U.S. Health-Care System Shaped COVID-19 Vaccine Hesitancy
- Find this author on Google Scholar
- Find this author on PubMed
- Search for this author on this site
- ORCID record for Amy Casselman-Hontalas
- Figures & Data
- Info & Metrics
This article explores the relationships between the American health-care system, trust in institutions, and decision-making processes that have affected COVID-19 vaccine uptake. Findings are based on an analysis of a nationally representative sample of 137 individuals who participated in semi-structured qualitative interviews during the rollout of the first publicly available vaccine in the first quarter of 2021. The vast majority of respondents reported negative experiences with American health care that predated the pandemic, which generated distrust in medical institutions, including hospitals, private health insurance corporations, the pharmaceutical industry, and related government institutions. The article considers the impact of institutional distrust on attitudes about vaccine uptake. Responses fell along a spectrum from vaccine refusal to vaccine acceptance. Sentiment across categories revealed a high degree of hesitancy framed in terms of institutional distrust. The data reveal a complex landscape of beliefs and perceptions, illustrating widespread hesitancy and ambivalence among participants.
- vaccine hesitancy
- public health
- health care
- health insurance
- institutions
- medical-industrial complex
The COVID-19 pandemic raises serious questions about how a health-care system that has historically left many uninsured and underinsured can manage a public health crisis. Interviews with participants in the American Voices Project (AVP), a nationally representative qualitative interview survey of Americans, revealed persistently high barriers to accessing high-quality affordable health care in the United States. Such barriers have engendered a sense of distrust in the U.S. health-care system and its associated institutions, including hospitals, private health insurance corporations, the pharmaceutical industry, and government institutions charged with regulating and delivering care. COVID-19 vaccination efforts in the United States and the responses to those efforts have demonstrated the lethal consequences of institutional distrust at a time when individuals are explicitly asked to place their confidence in public health guidance and medical interventions.
Even though much has been written about the formidable barriers to high-quality affordable health care in the United States, less is known about the relationship between these barriers and the decision-making processes surrounding COVID-19 vaccine uptake. Data from our sample reveal a long history of negative experiences with the American health-care system that predate the onset of the pandemic and are strongly correlated with institutional distrust and widespread skepticism of the COVID-19 vaccine. Such a correlation helps explain the high degree of hesitancy in our data, including among participants who stated that they would likely receive the vaccine. Further, our data show that pre-existing distrust in a wide range of health-care institutions was nearly universal and therefore pervasive across race, gender, class, and political affiliation. Thus, rather than lending evidence to a polarizing discourse that hinges on a pro- and anti-vax binary, the data reveal a complex landscape of beliefs and perceptions, illustrating widespread hesitancy and ambivalence among participants across various dispositions.
This article draws a through line between distrust in American institutions and COVID-19 vaccination beliefs and intentions. We present and discuss our findings in two phases. First, we explore participant interactions with the American health-care system, highlighting the sources and contours of distrust in the medical-industrial complex. The data indicate that negative experiences with American health-care institutions were well entrenched before the pandemic. Thus, we purposefully use the term distrust rather than mistrust because the former indicates a settled belief rather than generalized doubt (Jennings et al. 2021 ). Second, having mapped the pervasive sense of distrust in the very institutions that play the most critical roles in vaccine development and delivery, we then discuss our participants’ decision-making processes as they weighed the risks and benefits of vaccination. In their interviews, each of the 137 participants in our sample described their feelings about the newly developed COVID-19 vaccine as well as their intentions regarding vaccination. Combining attitudinal and behavioral data led us to develop a vaccine disposition typology onto which each participant was mapped (see table 1 ). This typology ranges from pro- to anti-COVID-19 vaccine uptake dispositions and features several degrees of hesitancy between the two extremes.
- View inline
- Download powerpoint
Vaccination Typology with Definitions and Examples
To operationalize vaccine hesitancy for our typology we borrowed from the work of Bipin Adhikari, Phaik Yeong Cheah, and Lorenz von Seidlein ( 2022 , 2), who define vaccine hesitancy as “a state of uncertainty in decision-making due to doubts about the benefits of vaccines, their safety and necessity; and is a transient stage where a candidate may weigh the risks versus benefits of more emotional aspects associated with vaccinations.” Unlike other descriptions that portray hesitancy in static terms, this definition captures the processual and transient nature of vaccine decision-making that we observed in participants as they described negotiating a barrage of institutional messaging while feeling heightened social pressure.
By considering respondent attitudes in the context of vaccine intentions, we were able to conduct a nuanced appraisal of decision-making that captured widespread ambivalence that might have otherwise been obscured. In categorizing participants into our vaccination disposition typology, we also tracked the reasons participants gave for their hesitancy. The most frequently cited reasons included a nonspecific general lack of trust, feeling that the development of the vaccine was rushed, concern over unforeseen side effects, too little information about the vaccine, and lack of concern about contracting COVID-19. With the exception of being unconcerned about contracting COVID-19, all reflect matters of institutional trust. Further, because many participants discussed multiple reasons, even those who claimed they were not concerned about contracting the virus also cited trust-related reasons (such as “I don’t really trust the vaccine and because I don’t think I’ll get COVID anyway it’s not worth the risk”). Thus, we find that institutional trust is salient to understanding COVID-19 vaccine hesitancy.
- LITERATURE REVIEW
Our analysis builds on research on trust and vaccines that has explored the dynamics that might have influenced respondents’ dispositions during the rollout of the first publicly available COVID-19 vaccine. Trust in individuals and institutions is central to the vaccine decision-making processes. Trust as a social phenomenon can be conceptualized as “a relationship that exists between individuals, as well as between individuals and a system, in which one party accepts a vulnerable position, assuming the best interests and competence of the other, in exchange for a reduction in decision complexity” (Verger and Dubé 2020 , 991). This definition demonstrates that trust can be both interpersonal and institutional and typically involves a level of risk which must be negotiated by a trusting party. Interpersonal trust is said to exist between individuals when one or more parties becomes vulnerable by placing their faith in another in order to gain a possible advantage (Spadaro et al. 2020 ). For our purposes, we might consider a layperson who does not have the medical training needed to empirically evaluate the risks and benefits of a particular vaccine. By placing their trust in a medical professional’s endorsement of a vaccine, a layperson benefits from reduced decision complexity but also risks falling victim to bad medical advice.
Institutional trust, defined as “the extent to which individuals accept and perceive institutions as benevolent, competent, reliable and responsible toward citizens,” offers similar risks and rewards (Spadaro et al. 2020 , 3). The American health-care system, in its capacity to provide lifesaving care, is a powerful locus where one might develop institutional trust. Yet such institutions may also deny or create barriers to access to care, provide care at an exorbitant cost to patients, or provide substandard care, all of which may undermine institutional trust. Therefore, determining the extent to which health-care institutions can be trusted as “benevolent, competent, reliable and responsible” may be fraught as individuals weigh the benefits and risks of their vulnerability to institutional power.
Despite the distinctions between the two forms, institutional trust is frequently enmeshed with interpersonal trust. Because institutions are ultimately composed of individuals, institutional trust is necessarily structured by the trustworthiness of individual actors (Blendon 2006 ). For example, Robert Blendon and John Benson ( 2022 ) cite a study indicating that the United States, when compared with peer nations, ranked near the bottom in trust in health-care institutions, with only 14 percent of Americans surveyed reporting that they trusted hospitals completely. Yet, in the same study, 84 percent of Americans reported that they trust their individual doctors completely. Here, high levels of interpersonal trust are constrained by what is ultimately an institutional project, illustrating the complex dynamics of trust as a multifaceted sociological phenomenon.
We also emphasize a temporal dimension of both interpersonal and institutional trust. In explicating trust within the interpersonal, dyadic context, Dmitry Khodyakov ( 2007 , 126) writes that “the decision to trust another person is made in the present and is affected by the partner’s reputation, which represents the past, and by the expectation of possible tangible and/or non-material rewards, which represents the future.” Thus we expand our definition of trust to conceptualize it as a process of “constant imaginative anticipation of the reliability of the other party’s actions” based on “the reputation of the partner and the actor, … the evaluation of current circumstances of action, … assumptions about the partner’s actions, and … the belief in the honesty and morality of the other side” (Khodyakov 2007 , 126). Such a conceptualization suggests that past experiences are instrumental in undermining or bolstering trust in both interpersonal and institutional contexts.
Similarly, Khodyakov ( 2007 ) distinguishes “thick” and “thin” as two variations of interpersonal trust. Thick interpersonal trust is defined as “the first type of trust people develop in their lives,” which is necessary for both “developing an optimistic attitude towards others” and making social interactions possible (120). By contrast, thin interpersonal trust involves “trusting members of out-groups” and is “riskier” than thick interpersonal trust because it hinges on forming “relationships with people whose real intentions may not be clear” (121). Accordingly, trustworthiness in the absence of previous relationships depends on two factors: “the image of intermediaries that the trustor relies on for obtaining information about trustees … and/or the trustworthiness of institutions that back up trustees” (122). To understand this point, one need only think about recommendations sought and given by trustworthy intermediaries for various service providers (legal counsel, mechanics, doctors, and so on). Thin interpersonal trust, then, depends significantly on the reputation of the trustee as well as that of the intermediary of trust (see Zucker 1986 ).
Beyond the interpersonal domain, scholarly inquiry into institutional trust should benefit contemporary society precisely because we heavily rely on the state and its institutions in our everyday lives. Further, as Geraint Parry ( 1976 ) explicates, the institutional trust held by an individual corresponds to the presumed efficacy of state institutions. Like the significance of the parties’ reputations in building thin interpersonal trust, institutional trust “depends on [institutions’] perceived legitimacy, technical competence, and ability to perform assigned duties efficiently” (Khodyakov 2007 , 123). As Khodyakov ( 2007 , 123) argues, “it is the impersonal nature of institutions that makes creation of institutional trust so difficult, because it is more problematic to trust some abstract principles or anonymous others who do not express any feelings and emotions.” One of the central goals of institutional trust, then, is to cultivate “voluntary deference to the decisions made by institutions and increase public compliance with existing [and we might add new] rules and regulations.”
Researchers have shown that trust plays a crucial role in gaining public support for vaccines, but no consensus has been reached regarding how trust should be assessed, the specific components of trust that should be considered, and the relationships that warrant investigation (Jamison, Quinn, and Freimuth 2019 ; Larson et al. 2014 ). This lack of consensus is not exclusive to vaccine-related studies but instead mirrors the inherent complexities associated with understanding the concept of trust. Clearly, though, trust in vaccines depends on both confidence in the vaccines themselves as products and trust in the system that is responsible for their production and distribution (De Freitas, Damion, and Han-I 2021 ; Jamison, Quinn, and Freimuth 2019 ).
To better understand the relationship between trust and vaccines, scholars have constructed models that capture factors that influence vaccine beliefs and behaviors (see, for example, Wiysonge et al. 2022 ; Verger and Dubé 2020 ; Dubé and MacDonald 2016 ). For example, the 3C model—which identifies three critical factors in vaccine hesitancy—parses vaccine attitudes, intentions, and dispositions into the following categories: complacency, the degree to which the disease is perceived as low-risk or the vaccine is perceived as having low efficacy; convenience, when behavior may be affected by logistical barriers; and confidence, when decision-making is based on perceived efficacy and trustworthiness (see Verger and Dubé 2020 ; Dubé and MacDonald 2016 ; MacDonald 2015 ). The 3C model is sometimes expanded to the 5C model, adding calculation (when decision-making rests on weighing the risks and benefits of a given vaccine) and collective responsibility (when behavior is influenced by one’s desire to contribute to the overall health of one’s community) as important factors that influence vaccine beliefs and behaviors (Wiysonge et al. 2022 ; Betsch et al. 2018 ).
The 5C framework includes factors such as individual beliefs, social dynamics, and institutional constraints, which together demonstrate that vaccine dispositions, including vaccine hesitancy, are “complex and context specific, varying across time [and] place” (World Health Organization quoted in Betsch et al. 2018 ). In line with Khodyakov’s notion of “trust as a process,” Ed Pertwee, Clarissa Simas, and Heidi Larson ( 2022 , 458) argue that vaccine hesitancy is “better conceived of as a decision-making process rather than a fixed set of beliefs.” An individual’s vaccine disposition may change over time and shift in various contexts, so scholars emphasize that expressing concern about a vaccine is not the same as assuming an anti-vaccination stance (Pertwee, Simas, and Larson 2022 ; Betsch et al. 2018 ; Dubé et al. 2013 ). Moreover, focusing on the processual nature of vaccine dispositions allows researchers to better understand how “cultural, temporal, and spatial” factors influence vaccine hesitancy (MacDonald 2015 ).
General vaccine-hesitancy literature offers practical tools such as the 3C and 5C models as well as theoretical frameworks that have significantly enhanced our understanding of COVID-19–specific phenomena. Theories of interpersonal trust in vaccine uptake are of particular interest, given that data show that trust between a patient and an individual care provider (such as a personal physician) is highly correlated with COVID-19 vaccine uptake (Karpman et al. 2021 ). Further, data show that COVID-19 vaccine intentions are affected by institutional trust in American health-care systems where a lack of trust in any or all components of this system can result in hesitancy and diminished compliance with recommended health practices (Blendon and Benson 2022 ; Bagasra, Doan, and Allen 2021 ).
- DATA AND METHODS
The data for this article are derived from the American Voices Project (AVP), which conducts in-depth interviews to offer a rich and comprehensive landscape of life across the United States. The AVP reflects a nationally representative sample of hundreds of American communities as well as a representative sample within each of the selected sites. The AVP used three-stage cluster sampling in which census tracts were selected by stratified sampling and captured key geographic areas as single-block groups were sampled within tracts to focus on well-defined communities. Tracts and block groups were then selected with a probability proportional to the poverty population to explore the everyday lives of low-income populations. Additionally, select middle- and high-income populations were sampled for comparison purposes and to capture an overview of American life.
Interviews reveal critical dimensions of everyday life, including aspects of family life, living situations, community, health, emotional well-being, cost of living, and income as well as political perceptions. The AVP includes a database of 1,613 transcribed interviews. The data used in this article stem from a subsample of respondents ( N = 198) interviewed between January 2021 and March 2021 during the health wave of interviews in which the AVP adjusted its protocol to better capture health-related issues. These health wave months marked a critical moment in which COVID-19 vaccines were becoming available to the American public for the first time. 1
To best capture participants’ decision-making processes, we excluded participants from the health wave interviews ( N = 198) when we were unable to discern their vaccine dispositions. Although some participants declined to answer questions about their vaccine dispositions, the majority of those excluded were interviewed using a protocol that did not include a specific question about vaccine attitudes or intentions. In some cases, we were able to include participants from this group if other areas of their interviews indicated clear dispositions. A total of sixty-one participants were excluded, leaving a vaccine subsample ( N = 137) on which our analysis is based. Respondents were assigned pseudonyms and, to protect their identities, inconsequential details from interview excerpts have been omitted or changed.
The vaccine subsample yielded a representative participant pool with diversity across race, gender, income, age, and political affiliations (see table 2 ). The subsample mirrored critical health-related demographics. For example, respondents reported that they had either received at least one dose of the COVID-19 vaccine or planned to receive it when it became available at rates comparable to the national rate of 47 percent. 2 Likewise, our respondents relied on public health insurance programs at rates on par with national data; 18.25 percent of AVP respondents in our sample were Medicare recipients compared with 18.4 percent of the U.S. population as a whole (see table 3 ; Keisler-Starkey and Bunch 2021 ). The only substantive difference between our sample and national statistics was the percentage of respondents who relied on private employer-based health insurance, 29.2 percent relative to 54.3 percent on the national level (U.S. Census Bureau 2021a ). Parity in public coverage rates indicate that the discrepancy in private coverage reflects classification rather than demographic differences. For confidentiality reasons, table cells containing fewer than eleven participants were collapsed into the Insured–Other category (see table 3 ). Doing so obscured subsets of participants whose insurance likely flowed from employer-based coverage. For example, young adults in our sample who stated that they were covered by a parent’s health insurance plan were classified as Insured–Other even though such coverage almost always flows from a parent’s employer-based private health insurance plan.
Demographics ( N = 137)
Health Insurance Coverage ( N = 137)
Data are drawn from participant interviews that were conducted by a diverse team of advanced degree holders as well as graduate students, college graduates, and undergraduates; all team members were selected through a highly competitive process and received additional intensive training in qualitative methods. Members of the team were also tasked with applying a basic codebook to the interviews using NVivo qualitative coding software. This codebook was generated by AVP leadership to flag broad themes related to health, including participant experiences with the health-care system, perceptions of the COVID-19 pandemic, and attitudes toward the newly developed COVID-19 vaccine.
We reviewed the transcribed interviews and previously coded data, analyzing the content inductively while developing a unique codebook to identify and categorize emerging themes. In addition to providing insight into how respondents perceived and interacted with American health-care institutions broadly, qualitative coding led us to develop a vaccine typology that categorized participants into one of five vaccine dispositions. We were frequently able to determine a respondent’s disposition based on the following interview question: “Some people are excited about the new COVID-19 vaccine, and others not so much. How about for you?” The open-ended nature of this question, crafted to avoid social desirability bias, frequently elicited statements of intent and captured hesitancy when it existed (for example, “I’m not really excited about it. I’ll probably get it, but I’m worried about the side effects”). That said, we did not assume that a participant’s answer to this question was dispositive. Because many participants discussed COVID-19 when responding to multiple questions, we relied on a holistic evaluation of a participant’s entire interview to classify their disposition. To ensure intercoder reliability, we developed a vaccination typology with definitions and examples (see table 1 ). Although our data are rich and support a nuanced analysis, this article is limited to the extent that it relies on interviews that we did not conduct using an interview protocol that we did not create. As a result, we were unable to tease out additional complexity, clarify ambiguous points, or explore the details of participants’ experiences more fully. Future or follow-up research should be conducted to corroborate our findings.
- SETTING THE STAGE OF DISTRUST
We can better understand the dynamics that influenced and continue to animate COVID-19 vaccination hesitancy by situating such discourses against the backdrop of individuals’ experiences and perceptions of the U.S. health-care system. In this section, we demonstrate how negative experiences with the system generated distrust in the very institutions that individuals were asked to entrust with their lives and the lives of their families.
At the time of their interviews, almost all of our study participants were enrolled in some form of institutional health-care coverage that generally fell into one of three categories: private employer-based coverage or public coverage through either Medicaid or Medicare (see table 3 ). Despite the diversity of health-care needs, access points, and types of insurance coverage, the vast majority of our participants expressed dissatisfaction with their experiences accessing health care. With the exception of respondents who enjoyed generous coverage through union benefits or who were covered by multiple policies, most individuals expressed frustration with various aspects of the health-care system. Respondents were exasperated by high co-pays and coinsurance, hidden costs and surprise billing, and lack of coverage for vision and dental care. Further, many were underinsured and found it difficult to pay both monthly premiums and medical bills that were generally not covered due to high deductibles. Many of these frustrations were directed at private insurance companies; however, participants also expressed dissatisfaction with other institutions such as hospitals and pharmaceutical corporations. Respondents also directed their frustrations at the government more broadly, both as a provider of health coverage in the form of Medicare and Medicaid and as the entity responsible for regulating private health insurers and the pharmaceutical industry.
Although most participants were covered by health insurance, many were still forced to forgo, delay, or ration care. Underinsured participants were covered by policies with both high premiums and high deductibles where they made large monthly payments for services that they still could not afford. Jennifer, a young, low-income white woman, said this of her mother:
She has not been to the doctor in a long time, because insurance is just too crazy. She has health insurance, so it’s kind of for emergencies. So, she won’t go to the doctor because it’s just too expensive. It’s just too expensive to go get a physical and do a [wellness] check. … But I know my mom was paying like $500 a month. And that was just for emergencies. … And it was kind of, it was more than our house payment. So, it’s kind of ridiculous.
Similarly, Susan, a low-income black woman in her sixties, explained, “it’s like we have insurance, but then I go to a doctor I have to pay a $400 deductible; $400, that’s a whole week’s pay. So it’s hard to stay healthy. So you let a lot of things slide, probably that you shouldn’t.” Despite paying for services that exceed the cost of a house payment or a week’s wages, Jennifer’s mother and Susan forwent the services that would help them “stay healthy.”
In the face of such challenges, participants made strategic calculations that included rationing care. For example, Jeff, a white man in his fifties, said:
My disability check does not go very far, and so I have had times that I ran out of [medication] and had to make our rations, make what I had last until payday or until I get the check. With my current [care provider], who also [treats] my [condition], it’s $300, but I can’t afford $300. So, I had to stop taking that medication. [There’s one specialty medication that I need to take or else I’ll die]. Everything else is icing on the cake.
Jeff’s remarks illustrate how negative experiences navigating health-care institutions, such as the Social Security Disability Insurance system, can generate feelings of distrust as individuals are forced to make difficult and life-compromising decisions about their health and well-being.
Although participants described positive interactions with individual medical professionals such as doctors and nurses, the hospitals and other facilities where they received care were often regarded as prioritizing profits over people. For example, when Tomás, a middle-income Hispanic man in his twenties, went to the emergency room for a serious injury, the institution’s priorities felt clear: “I’m bleeding, and they’re worried about me filling out some papers. I just took a deep breath, and I’m like, ‘Man, they’re more worried about money than my health.’” In addition to frustration with bureaucratic protocols, another thought loomed over him: “As I’m walking into the door, honest to God, I’m thinking, ‘And I might have to pay this big bill.’”
Echoing Tomás, Bill, a white man in his sixties, clearly indicated his disdain for and distrust in health-care institutions:
They’re all on quotas for how many minutes they’re going to spend with a patient. And really, it’s the bean counters running the system now; it’s really appalling. It seems that the first thing they do is a walletectomy, of course; they want to see your medical insurance card and your charge cards and whatnot. It seems like the system is geared towards extracting the maximum amount of money for the minimum amount of service, and really efficiently, so I’m not especially pleased with it. It’s all about hiding the cost so you don’t know how much you’re paying or who’s paying it. The whole insurance system is really very destructive in that regard: you don’t know what things cost, you don’t know what you’re really going to pay.
Here, Bill frames health-care institutions as being intentionally exploitative (“extracting the maximum amount of money for the minimum amount of service”) and opaque (“It’s all about hiding the cost”). His comments also indicate that he sees both service institutions and insurance corporations as enmeshed where the provider “hid[es] the cost” as part of an “insurance system that is really very destructive.”
Building on his earlier comments, Bill discussed his attitudes toward pharmaceutical companies, whom he viewed as “rip[ping] off” consumers. To illustrate his point, he discussed a lifesaving medication that was affordable until the patent was purchased by a pharmaceutical company: “The company bought the patents on them and jacked up the price that should not have been permitted; those executives should have been marched down to a parking lot and dealt with.” This comment exemplifies the distrust in the pharmaceutical industry that punctuates our data, and, when read with his earlier comments, reveals how some respondents regard the American health-care system as an industrial complex in which myriad institutions work together to confuse, exploit, and swindle citizens.
When discussing their general health-care experiences and the COVID-19 pandemic, many individuals directed their frustrations at politicians and the government. The majority of respondents did not reference specific people or point to particular laws when discussing their frustrations but instead expressed a general distrust in politicians and the U.S. government more broadly. As Lisa, a young white woman, noted, “I personally just find it incredibly horrible that we are in the middle of a global pandemic, and there’s still people who are—and by people I mean politicians who find it appropriate to say, ‘Yeah, well, I mean, health care is a privilege, not a right,’ … that’s just more of a societal America [that] does an atrocious job with our health care.”
Similarly, Barbara, a middle-aged white woman encountering difficulty enrolling in a public health-care program, felt that the government did not care about her or others: “You’re on your own, like too bad, even if you are applying for like disability, they don’t care, they do not care.” Barbara’s and Lisa’s testimonies illustrate some ways in which participants attribute barriers to accessing health care to the lack of competency (“an atrocious job with our health care”) and lack of concern (“they don’t care”) from the U.S. health-care system and the government more broadly.
Although participant dissatisfaction with health care was persistent and predated COVID-19, the general sense of institutional distrust became increasingly pronounced as respondents began discussing their experiences during the pandemic. A number of participants specifically linked their pre-existing institutional distrust with their assessment of the COVID-19 vaccine. The pharmaceutical companies, in their roles as manufacturers and distributors of the vaccine, and the government, in its roles of overseeing vaccine development and responding to the pandemic more broadly, were the two most frequently cited institutions by participants. For example, when asked about his vaccine intentions, Kyle, a white man in his forties, remarked, “I’m always skeptical of the companies that developed it and what they put out, because they’re in the process of trying to make money typically. So, anyone that’s doing something with a financial interest I’m like more skeptical of.”
Here, Kyle links his pre-existing distrust in corporations (“anyone that’s doing something with a financial interest”) to his specific distrust in the pharmaceutical companies responsible for producing the COVID-19 vaccine. Like Kyle, George, a white man in his sixties, considered his general distrust in the pharmaceutical industry as he contemplated receiving the COVID-19 vaccine: “Well, I would say in the light of the circumstance I’ll take it when I get a chance, but I’m not hugely excited about drug companies. I don’t, I don’t trust them. I don’t trust them, but in light of what’s going on, I don’t know what, what is the—what else should we do?”
In his interview, George later assessed the federal government’s competence at managing the pandemic: “I mean right now obviously the United States is the worst country in the world when it comes to handling this thing.” When we read these comments together, we can see how distrust in one institution (the pharmaceutical industry) can sometimes spill over to lack of trust in related institutions (the U.S. government). Further, George’s statements highlight how vaccine dispositions are more nuanced and less predictable than one might assume. Indeed, even though George states a clear intention to receive the vaccine (“I’ll take it when I get a chance”), his declaration is couched within comments that express his dissatisfaction, hesitancy, and lack of trust. Ultimately, his decision to be vaccinated does not depend on a positive assessment of the vaccine or the health-care institutions in charge of creating and disseminating it. Instead, it is informed by an overall sense of resignation (“What else should we do?”). Given George’s apathy for and distrust in multiple health-care institutions, one could easily imagine a scenario in which he instead chose to refuse the vaccine. His decision-making process illustrates the phenomenon that we discuss in the following section. Like many of his peers in this study, participants who either received or planned to receive the COVID-19 vaccine often expressed hesitancy. Further, the data show that discourse across the hesitant spectrum was remarkably similar.
- VACCINE DISCOURSE AND DECISION-MAKING IN THE AGE OF COVID-19
This section builds on the preceding discussion to further explore the impact of existing institutional distrust on COVID-19 dispositions using a novel vaccination typology (see table 1 ). Based on interview data that revealed their vaccine attitudes and behaviors, we assigned respondents to one of the following categories:
Pro-vax: Respondent had received the COVID-19 vaccine or planned to and did not express hesitancy.
Pro-vax hesitant: Respondent leaned toward receiving the COVID-19 vaccine but expressed hesitancy.
Undecided hesitant: Respondent was undecided about receiving the COVID-19 vaccine and expressed hesitancy.
Anti-vax hesitant: Respondent leaned away from receiving the COVID-19 vaccine and expressed hesitancy.
Anti-vax: Respondent had not and will not receive the COVID-19 vaccine and did not express hesitancy.
By mapping each participant onto this typology, we find that participant decision-making processes are nuanced and that attitudes overlap even between respondents with oppositional dispositions (see tables 1 and 4 ). Indeed, individuals of all vaccine dispositions expressed varying degrees of distrust in health-related institutions. First, we begin with a brief discussion of individuals who did not express hesitancy about receiving the vaccine ( N = 86). We then contrast these dispositions with a large cohort of respondents ( N = 51) who were vaccine hesitant. We end the section by outlining the tipping points that nudge hesitant respondents to adopt a pro-vax stance.
Vaccination Disposition ( N = 137)
As noted, pro-vax respondents had either received or planned to receive the COVID-19 vaccine and did not express hesitancy. Despite a lack of hesitation, many participants in the pro-vax sample ( N = 66) still considered the role of trust when discussing health-care institutions. This frequently came in the form of considering why others might opt out of vaccination. For example, Kayla, a middle-income white woman in her twenties, explained: “I’m excited about it. I’m like, give me a call, I’ll take it. I am not going to be someone to refuse this. I trust science, like, yeah, it hasn’t been researched that much yet, I don’t know, I trust the scientists who are working on it like 100 percent.” Here, Kayla acknowledged a lack of information about the vaccine (“it hasn’t been researched that much yet”), which could be cause for concern. However, Kayla’s personal trust in science as an institution eclipsed this potential risk. Notably, Kayla discussed institutional trust (“I trust science”) as well as trust in individuals (“I trust the scientists”). Although she does not mention specific individuals, such as a scientist whom she knows personally, her trust in scientists as individuals evinces the role of trusted intermediaries who facilitate institutional trust.
Unsurprisingly, on the other end of the spectrum, anti-vax individuals expressed starkly different views of the COVID-19 vaccine. Of the five dispositional categories, anti-vax participants ( N = 20) were the most likely to claim that COVID-19 is fake, overblown, or used to intentionally frighten Americans. Such attitudes rest on a fundamental distrust in the U.S. health-care system, signaling a strong relationship between trust in government institutions and vaccine disposition. For example, Gina, a low-income black woman in her sixties, said:
I don’t trust it. They came up with it too quick. … We don’t even know enough about what COVID is and then you’re going to take a vaccine for something you don’t even know. They ain’t explained it enough to me. First, I didn’t believe that it was actually real. Some people died of it. You know that they say people died. I don’t trust the COVID vaccine. I don’t think they researched it enough. They come up with it too quick.
Gina’s response illustrates how a lack of knowledge about the COVID-19 virus and the vaccine is linked to perceived inadequacies (“They came up with it too quick”), communication failures (“They ain’t explained it enough to me”), and general untrustworthiness in the U.S. health-care system (“You know that they say people died of it. I don’t trust the COVID vaccine”).
Finally, although rare in our sample, the racialized nature of anti-vax sentiments among some participants is noteworthy. Unlike demonstrably false conspiracy theories, the history in the United States of state-sponsored and state-sanctioned medical abuse of women, poor people, and people of color is documented (Wilson et al. 2023 ; Delgado 2020 ; INCITE! 2016 ; Washington 2006 ). Several anti-vax participants linked their historically informed, pre-existing distrust in the U.S. health-care system to their present-day vaccination dispositions. As Lydia, a low-income black woman in her sixties, explained: “Because of my history, African American history. Vaccines in America and just health care, being used as experimental pretty much. I can’t think of the word I want to say. But you know what I mean? I think about that, and they are very suspicious. … So, because we have a bad history in America, we still have a long way to go. I’m not interested in the vaccine.”
Several participants specifically referred to the Tuskegee Syphilis Study—when the federal government purposely withheld treatment for syphilis to study its progression in a sample of four hundred black men (Emanuel et al. 2008 ). James, a middle-income, multiracial man in his seventies, said this: “What really got to me though is that the [COVID-19 vaccine] experiment was after the syphilis experiment. So my whole thing is that this is the government. My whole thing is, well, shoot, they did this syphilis [experiment], and it was back again, they did it again to the same people, the group of people in Tuskegee.”
Like other respondents, James gave additional reasons for his anti-vax stance, including feeling that the development of the vaccine was rushed and that it would be impossible to anticipate its long-term effects: “Here, they [developed and manufactured the vaccine] in eight damn months, and that bothers me. Not to say it can’t be right, but the whole thing is you really don’t know what the side effects are. … But like I said, they have no idea what the outcome is going to be down the line.”
Not only does James attribute his anti-vax disposition to distrust in the U.S. government, he also expresses concern over hasty manufacturing and side effects that might emerge in time. Here, James articulates two of the most common refrains expressed by anti-vax participants and hesitant participants across the typological spectrum: that the vaccine was produced too quickly, and citizens lack the knowledge needed to make informed decisions.
Even though pro-vax and anti-vax respondents are diametrically opposed, both cohorts’ decision-making processes hinged on the presence or absence of trust in the U.S. health-care system. Similarly, in the subsample of hesitant respondents ( N = 51), pro-vax hesitant, undecided hesitant, and anti-vax hesitant individuals share similar trust-related reasons, or core beliefs, for their hesitancy. For these participants, the leading causes of hesitancy were not knowing enough about the vaccine to trust it and observing the seemingly rushed development of the vaccine. 3 That many COVID-19 vaccine-hesitant participants did not express concern over well-established vaccines (such as for influenza) highlights the value that respondents place on the additional data points that are available for products with established track records.
Hesitant individuals developed several strategies to manage their concerns about the COVID-19 vaccine, the most common being the wait-and-see approach articulated by participants in all three hesitant subgroups. This approach leaves open the possibility of being vaccinated at some future point after one is able to gather additional data about the vaccine’s safety and efficacy. Wendy, a low-income black woman in her forties whom we classified as pro-vax hesitant, stated, “I mean, I’m glad we have something that’s going to, that’s trying to clear this up. I’m just kind of waiting to see the outcome.” When the interviewer asked whether she would get the vaccine, she answered, “Debatable. It’s in the air. Like I said, I just want to see the outcome.” 4
Similarly, Ken, a white man in his sixties classified as anti-vax hesitant, questioned the efficacy of the vaccine and explained that he and his family would forgo getting the vaccine “until there’s more data”:
You still have to do the social distancing. You still have to keep wearing the mask. You can still pass it to somebody else. You can actually still get it because at least one person in the news has gotten it after being vaccinated. So, at this point in time, I don’t see the pluses of getting it. And my whole family feels the same way. None of us are going to get it until there’s more data out there to show that it’s actually doing something.
Notably, Wendy and Ken fall on opposite sides of the hesitancy spectrum (classified as pro-vax hesitant and anti-vax hesitant, respectively), yet use the same wait-and-see strategy in their vaccine decision-making process. That participants across the hesitancy spectrum frequently navigate uncertainty in similar ways makes clear that vaccine behaviors (that is, uptake and refusal) are mutable and subject to change.
As noted, we conceptualize vaccine hesitancy as a state of uncertainty in which an individual is actively engaged in weighing the risks and benefits of vaccination (Adhikari, Cheah, and Seidlein 2022 ). Thus, hesitancy is volatile and subject to outside influence. Our analysis reveals a number of factors that can nudge participants toward or against vaccine acceptance, creating pro-vax tipping points among hesitant respondents. As the extant literature would suggest, our data confirm that such tipping points emerge where trusted intermediaries have the opportunity to facilitate institutional trust. For example, Carmen, a Hispanic woman in her thirties, did not plan to receive the COVID-19 vaccine until an outreach worker visited her community to promote vaccination. Although Carmen remained uncommitted at the time of her interview, community outreach in the form of an intermediary shifted her disposition from anti-vax to undecided hesitant. She also indicated that, if the vaccine were easily accessible, she would be even more inclined to receive it. Thus, we should consider how the efficacy of trusted intermediaries is boosted when barriers to entry are lowered. Our data show that local clinics, pharmacies, and community centers acted as tipping point hubs for many respondents who would otherwise be more vaccine averse. Such micro-institutions appear to be effective because they offer easy vaccine access administered by trusted intermediaries (such as a local pharmacist) in familiar settings.
Frequently, individuals who attributed their hesitancy to lack of information about the vaccine noted that they wanted to do their own research before deciding. Although the concept of doing one’s own research is often derided by those who assume that the vaccine hesitant will find information from dubious sources, participants often used a variety of credible sources, including seeking out media representing diverse and balanced perspectives and consulting medical professionals to whom they have access. As Melissa, a middle-income Asian American woman, noted:
I’m feeling mostly optimistic about it. And yeah, I mean, at first, I was pessimistic but that was my misinformation, my misunderstanding. And I was until I came across in a news article about an MD PhD in Texas that was developing a low-cost vaccine, that got my attention because I realized that “Oh, wow. Okay, this vaccine is not really the product of operation warp speed as former President Trump tried to claim, or he did claim.” This vaccine is seventeen, eighteen years in the making.
Many participants were concerned about the apparent speed at which the COVID-19 vaccine was developed, but Melissa used news media featuring a credentialed expert to educate herself on the development of the vaccine. In doing so, her pessimism shifted toward optimism as she began to lean toward receiving the vaccine.
This article demonstrates how negative valuations steeped in past experiences with, and perceptions of, the U.S. health-care system generated distrust in institutions that seek to control public health crises. Regardless of insurance status, the vast majority of participants in this study were dissatisfied with the American health-care system. Because they had experienced this dissatisfaction for much of their lives, their trust in the system was compromised well before COVID-19 reached the United States. In the early days of the pandemic, most individuals watched an already overburdened health-care system strain under the weight of an unanticipated and unprecedented public health crisis. Despite their diverse backgrounds and experiences, as the first wave of COVID-19 vaccines became publicly available, all of our respondents were faced with the same question. Would they place their trust in the U.S. health-care system and its medical interventions to protect themselves and their loved ones from the COVID-19 virus? Here, like virtually all other Americans, our participants engaged their everyday life circumstances, social networks, past experiences, and available information to decide whether they would opt to receive the vaccine.
During the rollout of the first vaccine, institutional pressure to be vaccinated was high. Although many of our respondents expressed a clear desire to receive the vaccination ( N = 66) the majority were more reserved, with most expressing hesitancy or outright refusal ( N = 71). We found that participants’ vaccine dispositions resulted from a decision-making process that was social, cultural, and temporal. From a temporal standpoint, respondents drew on their pre-pandemic experiences with the American health-care system to evaluate potential future outcomes. Their dispositions at the time of the interview also reflected an appraisal of cultural messages communicated through media as well as the social influence of people in their immediate and extended social networks.
Even though medical professionals may feel frustrated by anti-vax or vaccine-hesitant attitudes and beliefs, our data underscore the importance of considering how information flows, and scientific knowledge in particular, are experienced by a variety of communities. Although the data are clear that COVID-19 vaccines are safe, effective, and necessary to protect the health of communities, we should be mindful of the context in which vaccine hesitancy arises and acknowledge the pervasiveness of vaccine hesitancy. Whereas a handful of individuals’ vaccine dispositions hinged on anecdotal information or dubious sources, these findings did not characterize the majority of participants’ core beliefs that led to vaccine hesitancy or refusal. In our review of 137 respondents, we found that vaccine opposition and hesitancy were rarely capricious but rather the outcome of agentic behavior amid various institutional constraints, including lack of institutional trust.
Our research makes both methodological and theoretical contributions to the extant COVID-19 literature. Methodologically, much of what we know about vaccine hesitancy relies on a large body of quantitative and survey data about general vaccine hesitancy as well as COVID-19-vaccine–specific hesitancy. We recognize that these datasets are rich sources of information but contend that qualitative data allow for more nuanced analyses that better capture decision-making processes. Frequently, quantitative projects rely on binary choices (such as “Have you taken the COVID-19 vaccine?” Yes/No), whereas surveys typically require a respondent to choose from a predetermined list of options (for example, “Which of the following options best describes your attitude toward the vaccine?”). In both cases, a respondent’s ability to give a full accounting of their perspective is limited. In contrast, qualitative projects allow respondents to express their experiences on their own terms, facilitating the detection of novel patterns that are otherwise obscured by quantitative methodology. This study moves beyond statistical trends to capture the discrete narratives and personal stories that shape worldviews.
Further, qualitative research on COVID-19 vaccine hesitancy typically relies on small sample sizes that are not generalizable. In contrast, our dataset is large and nationally representative and thus offers thorough insights into the American public’s attitudes and perspectives related to the COVID-19 pandemic. As we detail in the data and methods section, respondent demographics in our sample tracked closely with national data. Demographic similarities allow for greater generalizability in service of scaling our research in ways that exceed the scope of most qualitative projects. Having a high-quality, scalable qualitative dataset is especially valuable for inferences to national phenomena. Because participants were interviewed in the months surrounding the rollout of the first publicly available COVID-19 vaccine, their experiences speak to a wide audience because all Americans were undergoing similar processes in which they were evaluating existing information and forming vaccine intentions.
On a theoretical level, our findings further complicate discourses of polarization that place a wedge between pro-vax and anti-vax individuals. Although we were unsurprised that our data revealed a diversity of opinions related to the COVID-19 vaccine, we did not expect to find heightened levels of hesitancy among individuals on both sides of pro- and anti-vax equation. We found that participants who said that they would likely receive the vaccine expressed trust-related concerns that were remarkably similar to those expressed by respondents who said they would refuse or would likely refuse it. Indeed, pro-vax participants who were not hesitant about being vaccinated themselves validated the trust-related concerns their hesitant counterparts expressed. Hence, despite dominant media discourse that has framed vaccine dispositions as a fiercely pro- and anti-vax dichotomy, we found that most participants across all categories experienced similar decision-making processes. Relatedly, we found that participants in every category engaged in active, agentic decision-making processes rather than passively accepting institutional messaging. Thus, contrary to a simplistic narrative of a deeply divided nation, this study reveals the synergies and convergences in beliefs that point to widespread institutional distrust.
By drawing attention to vaccine hesitancy, we show that people’s stances are often more complicated than the pro- and anti-vax dichotomy suggests. The empirical richness of our data helped us explore the reasons, doubts, and fears that undergird these attitudes, offering a nuanced understanding of the factors influencing vaccine decisions. By unpacking and adding complexity to these narratives, we shed light on the salience of trust in the American public’s decision-making processes, including the relationship between pervasive barriers to high-quality affordable health care and vaccine hesitancy. Although we abjured making causal claims, our research documents the correlation between pre-existing distrust in American medical institutions and COVID-19 vaccine hesitancy that has both scholarly and real-world applications.
In examining the relationship between institutional trust and COVID-19 vaccine disposition, we were struck by the distribution of participants along demographic lines. We were surprised to find that each dispositional category was quite diverse. Although privacy constraints prevent us from disclosing the precise composition of each category within our vaccine typology, we find that all classifications include members of each racial, gender, income, and age demographic. This finding led us to conduct preliminary research on an additional variable—political affiliation—that was not part of our original research design. The scope of our research intentionally focuses on pre-pandemic distrust in health-care institutions rather than political affiliation as a corollary to COVID-19 vaccine disposition. Indeed, we find the former to be undertheorized relative to robust scholarly and media discourse centered on the relationship between political affiliation and vaccine disposition. Research on political affiliation generally concludes a negative correlation between Conservative or Republican identity and COVID-19 vaccine uptake (see, for example, Dolman et al. 2023 ; Albrecht 2022 ). Our observations about race, gender, class, and age diversity within vaccine typologies led us to question whether respondent data on political affiliation might differ from extant research that primarily relies on larger quantitative datasets.
A cursory analysis of the political affiliation of the participants in our sample produces findings that one might expect. 5 For example, the majority of those categorized as pro-vax are Democrats. Similarly, Democrats are less likely to be anti-vax than their Republican counterparts. Despite these findings, our data indicate that pre-existing distrust in medical institutions was nearly universal and thus transcends political affiliation. Although we do not refute studies that show that Democrats may be more trusting than Republicans in a variety of settings, our data document a shared experience that, by definition, crosses party lines. We also find it noteworthy that a substantive number of participants did not identify with a major party, signaling another form of ambivalence. Even though we find that the majority of Democrats were typed pro-vax, more than one-third were either vaccine hesitant or anti-vax. In contrast, more than one-third of Republicans were firmly pro-vax and fewer than one-third established themselves as anti-vax, figures that are respectively higher and lower than one might expect. Further—and perhaps most surprising—we find that anti-vax respondents are balanced across political affiliations. These findings point to the fact that hesitancy is widespread across the political spectrum in ways that may be paradoxical or unexpected. It is possible that this is due to sampling bias or a small sample size relative to most quantitative datasets. Nevertheless, we contend that these findings are intriguing and could prove to be fertile ground for additional research.
These conclusions make novel contributions to the relevant literature in that they demonstrate a through line between areas of study that remain balkanized in contemporary scholarly literature—namely the chronic, well-documented decades-long phenomenon of distrust in the U.S. health-care system and the onset of an unexpected and unprecedented pandemic. Finally, although COVID-19 vaccine literature discusses institutional trust, we find that it fails to adequately consider institutional distrust to be a condition already well entrenched at the onset of the pandemic. As a result, the relationship between the American health-care system, trust in American institutions, and decision-making processes vis-à-vis COVID-19 vaccine uptake remains undertheorized.
As health-care administrators and governmental institutions grapple with vaccine hesitancy, they should consider how their efforts either undermine or build trust. For example, top-down messaging from public health institutions often present complex and sometimes contradictory information that may confuse and overwhelm their audience and further undermine trust. When this happens, it is all too easy to link overwhelming feelings of confusion to extant feelings of distrust in the health-care system. If we accept the premise that trust in novel solutions is paramount to addressing public health crises, our data indicate that state actors and institutions must operate on a variety of levels to rebuild trust in a system that has failed and continues to fail the majority of Americans. This includes reconciling past medical injustices, removing barriers to accessing quality care, and restructuring institutions to make health care more affordable. Further, because many of our respondents described being influenced by social networks rather than institutional messaging, efforts toward rebuilding institutional trust must be prioritized.
↵ 1. Between December 2020 and March 2021, COVID-19 vaccines were becoming available to health-care workers, first responders, individuals in congregate settings, and the elderly in the United States (Mayo Clinic 2022 ).
↵ 2. In our sample, 47.45 percent of participants (surveyed between January 6 and March 24, 2021) reported they had received at least one dose of the COVID-19 vaccine or planned to receive their first dose when it became available. In March 2021, the U.S. Census reported that 47 percent of Americans had received at least one dose of the vaccine (U.S. Census Bureau 2021b ).
↵ 3. The COVID-19 vaccine is part of a class of mRNA vaccines that have been the subject of scientific research for three decades (Verbeke et al. 2021 ).
↵ 4. Although these statements seem to position Wendy in the undecided hesitant category, statements made elsewhere in her interview led us to classify her as pro-vax hesitant.
↵ 5. To protect respondent confidentiality, we excluded the number of participants of each political affiliation as it relates to their vaccine disposition. We did not include a table that illustrates our findings for the same reason.
- © 2024 Russell Sage Foundation. Casselman-Hontalas, Amy, Dominique Adams-Santos, and Celeste Watkins-Hayes. 2024. “Discourses of Distrust: How Lack of Trust in the U.S. Health-Care System Shaped COVID-19 Vaccine Hesitancy.” RSF: The Russell Sage Foundation Journal of the Social Sciences 10(4): 154–72. https://doi.org/10.7758/RSF.2024.10.4.07 . Direct correspondence to: Amy Casselman-Hontalas, at amylcass{at}stanford.edu , Stanford University, 450 Jane Stanford Way, Building 120, Room 160, Stanford, CA, 94305-2047, United States.
Open Access Policy: RSF: The Russell Sage Foundation Journal of the Social Sciences is an open access journal. This article is published under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
- Adhikari , Bipin ,
- Phaik Yeong Cheah , and
- Lorenz von Seidlein
- Albrecht , Don
- Bagasra , Anisah B .,
- Sara Doan , and
- Christopher T . Allen
- Betsch , Cornelia ,
- Philipp Schmid ,
- Dorothee Heinemeier ,
- Lars Korn ,
- Cindy Holtmann , and
- Robert Böhm
- Blendon , Robert J ., and
- John M . Benson
- David A . Shore
- Blendon , Robert J
- De Freitas , Loren ,
- Basdeo Damion , and
- Delgado , Melvin
- Dolman , Andrew J .,
- Timothy Fraser ,
- Costas Panagopoulos ,
- Daniel P . Aldrich , and
- Dubé , Eve ,
- Caroline Laberge ,
- Maryse Guay ,
- Paul Bramadat ,
- Réal Roy , and
- Julie A . Bettinger
- Barry R . Bloom and
- Paul-Henri Lambert
- Dubé , Eve , and
- Noni E . MacDonald
- Emanuel , Ezekiel J .,
- Christine C . Grady ,
- Robert A . Crouch ,
- Reidar K . Lie ,
- Franklin G . Miller , and
- David D . Wendler
- INCITE! Women of Color Against Violence
- Jamison , Amelia M .,
- Sandra Crouse Quinn , and
- Vicki S . Freimuth
- Jennings , Will ,
- Gerry Stoker ,
- Viktor Valgarðsson ,
- Daniel Devine , and
- Jennifer Gaskell
- Karpman , Michael ,
- Genevieve M . Kenney ,
- Stephen Zuckerman ,
- Dulce Gonzalez , and
- Brigette Courtot
- Keisler-Starkey , Katherine , and
- Lisa N . Bunch
- Khodyakov , Dmitry
- Larson , Heidi J .,
- Caitlin Jarrett ,
- Elizabeth Eckersberger ,
- David M . Smith , and
- Pauline Paterson
- MacDonald , Noni E
- Mayo Clinic
- Parry , Geraint
- Pertwee , Ed ,
- Clarissa Simas , and
- Heidi J . Larson
- Spadaro , Giuliana ,
- Katharina Gangl ,
- Jan-Willem Van Prooijen ,
- Paul A. M . Van Lange , and
- Cristina O . Mosso
- U.S. Census Bureau
- Verbeke , Rein ,
- Ine Lentacker ,
- Stefaan C. De Smedt , and
- Heleen Dewitte
- Verger Pierre , and
- Washington , Harriet. A
- Wilson , Betty L .,
- Julisa Tindall ,
- Denetra Walker , and
- Angela M . Smith
- Wiysonge , Charles Shey ,
- Duduzile Ndwandwe ,
- Jill Ryan ,
- Anelisa Jaca ,
- Oumarou Batouré ,
- Blanche-Philomene Melanga Anya , and
- Sara Cooper
- Zucker , Lynne
In this issue

- Table of Contents
- Table of Contents (PDF)
- Cover (PDF)
- Index by author
- Front Matter (PDF)
Thank you for your interest in spreading the word on RSF: The Russell Sage Foundation Journal of the Social Sciences.
NOTE: We only request your email address so that the person you are recommending the page to knows that you wanted them to see it, and that it is not junk mail. We do not capture any email address.
Citation Manager Formats
- EndNote (tagged)
- EndNote 8 (xml)
- RefWorks Tagged
- Ref Manager

- Tweet Widget
- Facebook Like
- Google Plus One
Jump to section
Related articles.
- No related articles found.
- Google Scholar
Cited By...
- No citing articles found.
Similar Articles
We Trust in Human Precision
20,000+ Professional Language Experts Ready to Help. Expertise in a variety of Niches.
API Solutions
- API Pricing
- Cost estimate
- Customer loyalty program
- Educational Discount
- Non-Profit Discount
- Green Initiative Discount1
Value-Driven Pricing
Unmatched expertise at affordable rates tailored for your needs. Our services empower you to boost your productivity.
- Special Discounts
- Enterprise transcription solutions
- Enterprise translation solutions
- Transcription/Caption API
- AI Transcription Proofreading API
Trusted by Global Leaders
GoTranscript is the chosen service for top media organizations, universities, and Fortune 50 companies.
GoTranscript
One of the Largest Online Transcription and Translation Agencies in the World. Founded in 2005.
Speaker 1: Let's be real, if you received a dollar every time someone told you to do your research before an interview, you'd have enough money to never have to job search again. Okay, maybe the amount would need to be slightly higher, but the fact remains that everyone tells you to do research, but no one walks you through the specific steps to take. In this video, I share three practical ways to do research that will help you find the most relevant, the most up-to-date information on the company and role that you're applying for. I'll also walk you through some specific situations to show how best to use all that information you just found to impress the interviewer. So let's get started. As you go through the three tips, it's important to remember how you use the findings from the research you did shouldn't just be limited to the answers you give during the interview, but rather also at the beginning of the interview where there might be some small talk and at the end where you should be asking meaningful questions directed at the interviewer. Don't worry if that sounds new to you, I'll be giving concrete examples as we go through each tip. So without further ado, let's start with interview research tip number one. Use Google Alerts to stay up to date on your target company's latest news and job postings. Google Alerts is a free tool that's extremely simple to use. You just set it up once and let it run automatically. In addition, by using a few simple search operators along with the name of the company, you turn this free tool into sort of a personal news assistant that provides you with regular updates. Let me share a few of my favorite examples. Example number one, if you type the job function in quotation marks, followed by the site search operator, you'll be alerted whenever a new job posting in that team is listed on their official careers page. One thing to note is that different companies obviously have different website URLs. So you just need to search for that company's official career page once, copy and paste it here and just let it run. For example, for Google, that URL would be careers.google.com, whereas for Tesla, it would be tesla.com slash careers. If you really want to get fancy, you can type in a broader organization in that company, followed by an asterisk, like marketing asterisk Tesla, site tesla.com slash careers, and you only receive job alerts if a marketing role opens up. Similarly, if you want to cover all your bases, you can simply input the company name, let's say Tesla, followed by site linkedin.com or site indeed.com to see the job postings there as well. An often overlooked fact is that the first application received is often read in more detail than later applications. So with Google alerts, you can be that early bird that gets the worm, but no one really thinks about the early worm. Second example, if you type in the company name followed by the word competition, you'll receive alerts whenever the company is mentioned in a competitive context in the news and blog posts. Not only will this give you a good idea of who their closest competitors are, but will also point you to well-written articles on industry trends and on challenges your target company might be facing. This is actually also a great example of how, while you probably can't use all that information in your answers to the standard interview questions, you can definitely bring that up in other scenarios to show the interviewer you've been doing your homework. For example, in this Apple Spotify case, if you're interviewing with Apple, you might bring this up during the course of small talk and say something like this. Oh, and congratulations, by the way, on the acquisition of Scout FM. It seems like you guys are really doubling down on the AI podcast bet. Alternatively, if you're interviewing with Spotify, this might be a really good question to ask at the end of the interview. So I saw that Apple recently made a strategic purchase of Scout FM. I'm curious as to how that impacts Spotify's business strategy for next year. And number three, if you type in the company name, followed by the words quarterly earnings, you start to receive more financial-oriented alerts. This is useful if you're interviewing for financial institutions like banks, private equities, and hedge funds, and you're gonna be covering specific verticals like energy or tech. Or if you're accounting for a sales finance or an internal investment position at a publicly listed firm and would like to learn more about the company's financial health. The last thing I wanna point out is that these alerts are only useful if you read them. So I highly recommend you set up one or two and read them on a daily or weekly basis instead of setting up 10 at once and having your inbox completely overwhelmed. If you found this first tip helpful, I actually have a Facebook group where I share exclusive weekly tips. Consider joining if you haven't already. I'll link it down below. Interview research tip number two, use Google Trends to understand how demand for the target company's product has changed over time. Google Trends is another free tool provided by Google, hashtag not sponsored, that's really popular with research analysts, but can be used for job search and interviews as well. Jumping straight into a simple example, let's say you're interviewing with Tesla or any automaker that manufactures electric vehicles. If I type in electric cars on Google Trends and show results for the past five years, you'll see this graph. It doesn't take a genius to figure out that when COVID hit around March in the United States, demand for electric cars decreased sharply alongside many other products. However, an interesting insight you might draw from this five-year data is that fundamentally, user interest in electric cars and renewable energy is on the rise. And when COVID is inevitably over, the long-term outlook for the industry is extremely positive. Much like how smart investors look at the fundamentals of a company when making a stock purchase decision as opposed to isolated incidents, you can use Google Trends to learn more about the direction that user behavior is moving towards. On a more practical level, I can easily see candidates using this information when faced with the common why do you wanna work here interview question. You can say something like, funnily enough, I was playing around with Google Trends when I was doing my research and found that although there's a slight decrease in demand for electric cars at the start of 2020, I see that user interest has been growing steadily year on year for the past five years. With climate change and renewable energy being top of mind for many people, I'm certain that electric vehicles and similar innovations are here to stay. And with Tesla being at the forefront of the EV industry, I'm extremely excited to be able to bring my background and experiences to this role. Pro tip, you're usually able to uncover some very interesting insights if we do a side-by-side comparison of your target company's product with that of a competitor. For example, if you're interviewing for a business role at Google, you might learn through a Google alert you set up from tip number one, that over 70% of our 2020 Q2 revenue came from our Google ads business. Taking that a step further, let's say you decide to compare interest for Google ads to that of Facebook ads, and you see this following graph. Other than perhaps noticing Google ads started to outperform Facebook ads around the same time Jeff joined the product marketing team in 2018. This might be another great question to ask at the end of your interview. What drove the increase in user interest for Google ads versus Facebook ads in 2018? Was there simply a product update? Or did Google run a large-scale marketing campaign to raise brand awareness? Let me know down in the comments below the two or more products you might wanna search for on Google Trends to compare their respective performances. What'd you find? Interview research tip number three, use the Evolve Career Library to get access to exclusive reports and reviews on your target company. This tip is mainly for college students because most universities have access to vault.com's premium databases, and that premium content is a main differentiator between vault.com and free websites like Glassdoor and Indeed. I have lost access to the premium content since graduation, but I do distinctly remember reports like vault's verdict. I think this is where the writers would do primary and secondary research first, and then write a very comprehensive summary that is centralized in one location. But the free version has benefits as well. If you go to Career Advice section and click on Research Industries, and let's just click on Best Industries for Undergraduates and choose the number one energy industry as an example. And then we go to Overview. This provides a very good snapshot of the pros and cons of the industry that again, provides you with talking points for the interview. Something I found to be very interesting is this Defining Events section. Yes, at first glance, it's very, very wordy, and even talks about historical events from the 18th and 19th centuries. Probably too dry for 99% of us. However, if you scroll to the very bottom, you will see how current policies have shaped the industry thus far. For example, this paragraph here shows how this US president has had a major effect on the US energy policy over the past four years. And without touching on politics too much, this information can be used to ask another question to the interviewer. Something along the lines of, how would the current energy policies affect the electric vehicle industry for the next five years? So as you can see, even if you don't have access to the premium content, the free resources are still quite helpful. All right, there you have it. Three practical tips you can use the next time you do research for a job interview. Hopefully compared to some of the other articles and videos out there, this step-by-step research guide you should follow before your first interview showed you number one, where to find all this relevant information. And number two, how to use it throughout the interview process. Please give this video a like if you found it helpful and let me know down in the comments below if you have any questions. Subscribe if you haven't already. See you on the next video. And in the meantime, have a great one.

Information
- Author Services
Initiatives
You are accessing a machine-readable page. In order to be human-readable, please install an RSS reader.
All articles published by MDPI are made immediately available worldwide under an open access license. No special permission is required to reuse all or part of the article published by MDPI, including figures and tables. For articles published under an open access Creative Common CC BY license, any part of the article may be reused without permission provided that the original article is clearly cited. For more information, please refer to https://www.mdpi.com/openaccess .
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for future research directions and describes possible research applications.
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive positive feedback from the reviewers.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world. Editors select a small number of articles recently published in the journal that they believe will be particularly interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the most exciting work published in the various research areas of the journal.
Original Submission Date Received: .
- Active Journals
- Find a Journal
- Proceedings Series
- For Authors
- For Reviewers
- For Editors
- For Librarians
- For Publishers
- For Societies
- For Conference Organizers
- Open Access Policy
- Institutional Open Access Program
- Special Issues Guidelines
- Editorial Process
- Research and Publication Ethics
- Article Processing Charges
- Testimonials
- Preprints.org
- SciProfiles
- Encyclopedia
Article Menu
- Subscribe SciFeed
- Recommended Articles
- Author Biographies
- Google Scholar
- on Google Scholar
- Table of Contents
Find support for a specific problem in the support section of our website.
Please let us know what you think of our products and services.
Visit our dedicated information section to learn more about MDPI.
JSmol Viewer
‘if you do not write, you dry up’: tensions in teacher educator research and academic writing.

1. Introduction
1.1. teacher education in israel, 1.2. challenges for teacher educator writers.
The most frequently reported stressor for teacher educators was workload intensification, followed by university policy, processes, and procedures. Factors found to decrease teacher educator wellbeing included: job insecurity, excessive workload, supporting student wellbeing, perceived lack of institutional support, and teacher-researcher role conflict. (p. 12)
1.3. Institutional Ethnography
2. materials and methods, 2.1. participants.
| Neta | Professor |
| Hanny | Professor |
| May | Senior lecturer |
| Iris | Senior lecturer |
| Zohar | Professor |
| Moran | Professor |
| Tal | Senior lecturer |
| Ori | Non-academic ranking |
2.3. Data Analysis
2.4. ethical considerations, 2.5. researcher positioning, 3.1. the importance of academic activity for institutional prosperity, 3.1.1. the institutional structure, 3.1.2. improving teaching.
Doing research requires you to be renewed, to change all the time … You can see the difference between faculty who are active researchers and those who aren’t. Researchers’ syllabuses are up-to-date and change all the time. Others can stick with the same syllabus for a decade, and they won’t change a letter.
People should be up to date. The more you research and write, the more you are exposed, a thousand times more, and you are a thousand times better as a lecturer. A thousand times better. And people look up to you.
You can’t talk about applied research without being an applied researcher. That means that you can’t talk about soccer without being a player. A player needs to be active. To just be a trainer, a coach, without being a player … You need to be an active player who is developing … It is unquestionable!
One of my aims is to put as many programs as possible into the research stream with a thesis … We have four programs out of nine with temporary or permanent authorisation to require a thesis … With a thesis it is easier for our students to continue to a doctorate. Today, most … finish with practical term papers. That means an additional year of study and a thesis, and then they can continue to doctoral studies, and not in all universities … Eight to ten per cent continue to doctoral studies; I want them to have a good beginning so that they can come to the university with their heads high and join the most advanced programs.
3.1.3. Knowledge Generation
A separation of authorities between creators of knowledge and disseminators of knowledge. That means that educators are a kind of passive hose which passes on knowledge developed somewhere else … When we write about our research, we join a professional milieu which generates and develops knowledge.
… they fill a void in Israeli research as they research issues relevant to the field. They are at the junction because universities are too distant for a thousand and one reasons … The research of college faculty can develop a unique niche because we deal with teacher education and are connected to schools.
3.2. Difficulties in Academic Scholarship Experienced by Teacher Educators
3.2.1. academic background.
People don’t finish their studies and arrive here; they’ve usually progressed in educational or other fields; they come here with life achievements. They almost never begin here when they are very young. The percentage of people who arrive here from the field, from schools, is very high.
The work, the time, and the knowledge that publication requires … it’s difficult, and it doesn’t matter if you are a good educator or not … There are things you need to know, and nobody teaches you them … you learn them from personal experience; there are some that the process finishes them off and others who grow from it.
There are people in the college who are wonderful researchers, but the moment they sit down and work on publishing, it doesn’t work; they can’t do it. They can teach research methodology well, but they can’t take their research and get it published. It doesn’t work.
The longer people drag their feet after completing their doctorate, the worse their situation is … there is a handful of people who manage to progress after a break, but it is really, really difficult; it’s carving in a mountain … it is very, very difficult, and most get stuck and don’t succeed.
It’s Neta’s, my, the department chairs’, and the deans’ role to run after faculty … to push them, and push them, and push. I admit that sometimes, this leads to despair. People say, ‘I didn’t make any progress, I didn’t succeed, I didn’t move forward, I didn’t make it’. After three or four answers like that, I don’t bother.
3.2.2. Employment Scheme
It creates a situation where faculty members can’t make a living respectfully, even when employed full-time. They need to work in various other places … Based on sixteen teaching hours per week, with meagre wages, the chance of successfully engaging in research seriously and intensively is very low. If we want to be cynical, we can say that teaching in the college is approximately seven months of the year, then there are free months, so if people really want to find the time for research, they can. [Laughing] Of course, if they have to work in other jobs … when you teach sixteen weekly hours, you have to prepare many courses and grade many exams—it is all very, very difficult.
When you only give people third—or half-time employment, with very, very few hours, they aren’t even part of the group eligible to receive the resources. Until they have tenure, they can’t even reach the threshold of receiving resources from the college, even if they are really suitable for writing and academic promotion.
It’s also a matter of motivation and priorities. Don’t tell yourself the stories that half of the faculty, or even more, tell themselves. ‘How can I do research?’ ‘It’s not comfortable!’ Yes, we do teach a lot, but if you want to, it’s possible.
“ They are mainly women; most of the faculty here are women ”, Ori explained. Most teacher educators employed in the college are women, many with additional carer roles. They usually have less time and ability to reach self-realisation, and their salaries are low. Moran stressed, “ Their salaries are determined by what is called the ‘ranking of educational employees’; it’s the same collective agreement as schoolteachers, with nuances for colleges … It’s not really academia. It’s not the Council of Higher Education … ”. Zohar also acknowledged the role of the teacher educators’ families and the importance of their support in academic writing and promotion. “ There are some who succeed and others who don’t … I do not doubt that the support of the family environment and family expectations (if they want Mum to progress) make it easier ”.
3.2.3. Financial Resources
They always have groups of master’s and doctoral students; that’s firepower, crazy. We don’t have that at all. A few people here manage to do it a little by managing themselves wisely in the master’s program. Otherwise … you’re alone; with the loneliness, we don’t have research students here at all, and it significantly delays any progress.
3.2.4. Changing and Blurry College Agendas
There is an expectation that teacher educators progress and research. There are presidents who are more and those who are less, but there is an expectation to research, write, and progress. [The previous president] said it out loud, ‘It’s important. I want to promote the faculty academically’.
In the past, there was some confusion between those who wanted this to be an academic place, like a university and those who didn’t really want that. In that gap, there are many grey areas that aren’t solved and aren’t managed.
There is no agenda; the college doesn’t have any organised expectations [of new faculty]. Look at yourself. Has anyone ever told you what you have to do? Did they when they employed you? You’re nice, serious, okay, let’s move on. That’s how it works …. We don’t even have an organised index, not for requirements and not even for development to show people this is the direction. We don’t have it, and I think we should develop it. There are department chairs that it is important to them and others that it is less important to them. There are some that it is most important to them that everyone is nice.
If two people apply for a position, and one writes and the other doesn’t, the writer would be accepted … but it’s not written anywhere, and there is no organized format. We need to create an academic, not just an administrative, process of absorbing faculty. It needs to be much clearer, defined, and directed.
3.3. Institutional Support for Research and Writing
In reality, there is endless support; you only need to come and take it … The college gives a tremendous amount, more than any of the other colleges of education; I say that with full responsibility; I checked … and we give it to people without academic rankings as well.
Our research authority has always been an ‘institution’ compared to other colleges of education. It’s a kind of anchor that really supports the faculty members who want to do research and reach promotion … and in the end, the support bears fruit: very impressive research studies and promotions.
3.3.1. Research Funds
Do you know what it means to receive a grant? In most cases, you won’t get it. So here they only ask you for a declaration of intention, ‘This is what I’m planning to do …’, and then, of course, you must show that you have done something …. I think it is simple, one page in Hebrew, not more than that, a declaration of intention.
It’s easy for people not to notice. I said to one of the department chairs, ‘I can’t believe you haven’t applied’; she simply hadn’t noticed. It’s a shame … I have always been very active and understood what I am eligible for. There is no way I would miss funds, ever.
3.3.2. Research Groups and Programmes
3.3.3. consultancy and mentoring.
There is always someone you can talk to, even on short notice. I have sent many people to Zohar, and she gives you exactly what comes next and what you need to accomplish. People aren’t getting lost because of a lack of information. When they express interest, the college is very organised in what it provides … I think that gives a good feeling.
There is a lot to be satisfied with, the productivity, the doing, and the energy, but it is still saved for a limited group. I don’t know exactly how many, but approximately one hundred faculty members move around the research authority. They know how to respond to calls for papers and grants and are active. A large group isn’t there and doesn’t see themselves as belonging there. In short, I would be happy to see that grow if we could see it grow this year to 110 and next year to 120. I hope we are going in that direction.
4. Discussion
4.1. the conflict between institutional and individual advancements, 4.2. the structure of employment, 4.3. implications, 4.4. future research directions, author contributions, institutional review board statement, informed consent statement, data availability statement, conflicts of interest.
- Snow, J.L.; Jacobs, J.; Pignatosi, F.; Norman, P.; Rust, F.; Yendol-Hoppey, D.; Naiditch, F.; Nepstad, C.; Roosevelt, D.; Pointer-Mace, D.H.; et al. Making the Invisible Visible: Identifying Shared Functions that Enable the Complex Work of University-based Teacher Educators. Stud. Teach. Educ. 2023 , 19 , 351–375. [ Google Scholar ] [ CrossRef ]
- Ataş, U.; Daloğlu, A.; Hildén, R.K. Teacher educators in Finland and Turkey: Their roles, knowledge base, and professional development profiles. Eur. J. Teach. Educ. 2021 , 46 , 727–745. [ Google Scholar ] [ CrossRef ]
- Kosnik, C.; Menna, L.; Dharamshi, P. Displaced academics: Intended and unintended consequences of the changing landscape of teacher education. Eur. J. Teach. Educ. 2020 , 45 , 127–149. [ Google Scholar ] [ CrossRef ]
- MacPhail, A.; Ulvik, M.; Guberman, A.; Czerniawski, G.; Oolbekkink-Marchand, H.; Bain, Y. The professional development of higher education-based teacher educators: Needs and realities. Prof. Dev. Educ. 2018 , 45 , 848–861. [ Google Scholar ] [ CrossRef ]
- Turner, K.; Garvis, S. Teacher Educator Wellbeing, Stress and Burnout: A Scoping Review. Educ. Sci. 2023 , 13 , 351. [ Google Scholar ] [ CrossRef ]
- Parr, G.; Bulfin, S.; Diamond, F.; Wood, N.; Owen, C. The becoming of English teacher educators in Australia: A cross-generational reflexive inquiry. Oxf. Rev. Educ. 2019 , 46 , 238–256. [ Google Scholar ] [ CrossRef ]
- Ian, M. Teacher education research in the twenty-first century. In The Palgrave Handbook of Teacher Education ; Ian, M., Ed.; Palgrave Macmillan: London, UK, 2023; pp. 4–31. Available online: https://link.springer.com/referencework/10.1007/978-3-031-16193-3 (accessed on 23 August 2024).
- Tack, H.; Guberman, A.; MacPhail, A.; Vanderlinde, R. Higher education-based teacher educators’ researcherly disposition: An international perspective. Eur. J. Teach. Educ. 2023 , 1–13. [ Google Scholar ] [ CrossRef ]
- Guberman, A.; Mcdossi, O. Israeli teacher educators’ perceptions of their professional development paths in teaching, research and institutional leadership. Eur. J. Teach. Educ. 2019 , 42 , 507–522. [ Google Scholar ] [ CrossRef ]
- Ariav, T. Teacher education: The situation in the world and in Israel a look to the future. In The Crisis in Teacher Education: Reasons, Problems and Possible Solutions [In Hebrew] ; Van Leer Jerusalem Institute and Hakibbutz Hameuchad Publishing House: Jerusalem, Israel, 2008; pp. 19–55. [ Google Scholar ]
- Yogev, S.; Yogev, A. Teacher educators as researchers: A profile of research in Israeli teacher colleges versus university departments of education. Teach. Teach. Educ. 2006 , 22 , 32–41. [ Google Scholar ] [ CrossRef ]
- Aharonian, N. Teacher educators in an academic writing community: Fostering agency and well-being (submitted for publication).
- Vininger, A. Academic Institutions for Teacher Training: General Review. Presented to the Committee for Education, Culture, and Sport. Knesset Website. Israeli Ministry of Education: Israel, 2018. Available online: https://fs.knesset.gov.il/globaldocs/MMM/976403e8-19c2-e711-80de-00155d0a0235/2_976403e8-19c2-e711-80de-00155d0a0235_11_10529.pdf (accessed on 30 July 2024).
- Nasser-Abu Alhija, F.M.; Majdob, A. Predictors of teacher educators’ research productivity. Aust. J. Teach. Educ. 2017 , 42 , 34–51. [ Google Scholar ] [ CrossRef ]
- Gutman, M. From teacher to senior teacher educator: Exploring the teaching-research nexus in Israeli Academic Colleges of Education. J. Educ. Teach. Int. Res. Pedagog. 2021 , 47 , 439–453. [ Google Scholar ] [ CrossRef ]
- Cochran-Smith, M.; Grudnoff, L.; Orland-Barak, L.; Smith, K. Educating teacher educators: International perspectives. New Educ. 2019 , 16 , 5–24. [ Google Scholar ] [ CrossRef ]
- Ariav, T.; Kfir, D.; Feigin, N. The ‘academization’ of teacher education in Israel. Teach. Educ. 1993 , 5 , 151–161. [ Google Scholar ] [ CrossRef ]
- Gutman, M. “Balance as a way of lifework”: Early career choices among Israeli senior teacher educators. Teach. Educ. 2020 , 33 , 1–12. [ Google Scholar ] [ CrossRef ]
- Katz, E.; Coleman, M. The growing importance of research at academic colleges of education in Israel. Educ. + Train. 2001 , 43 , 82–93. [ Google Scholar ] [ CrossRef ]
- Julien, K.; Beres, J. Cheaper than therapy: The unexpected benefits and challenges of an academic writing partnership. In Critical Collaborative Communities ; Brill: Leiden, The Netherlands, 2019; pp. 3–16. [ Google Scholar ] [ CrossRef ]
- Steadman, C. Remembering and anticipating researcher vulnerability: An autoethnographic tale. J. Mark. Manag. 2023 , 39 , 807–828. [ Google Scholar ] [ CrossRef ]
- Loughran, J. Professionally Developing as a Teacher Educator. J. Teach. Educ. 2014 , 65 , 271–283. [ Google Scholar ] [ CrossRef ]
- Malm, B. On the complexities of educating student teachers: Teacher educators’ views on contemporary challenges to their profession. JET J. Educ. Teach./J. Educ. Teach. 2020 , 46 , 351–364. [ Google Scholar ] [ CrossRef ]
- Knowles, G.; Cole, A.; Sumsion, J. Modifying Conditions of Researching in Teacher Education Institutions. Teach. Educ. Q. 2000 , 27 , 7–13. Available online: https://www.jstor.org/stable/i23478080 (accessed on 21 November 2021).
- Smith, K.; Flores, M.A. Teacher educators as teachers and as researchers. Eur. J. Teach. Educ. 2019 , 42 , 429–432. [ Google Scholar ] [ CrossRef ]
- Nicholson, L.J.; Lander, V. Control beliefs of teacher educators regarding their research engagement. Educ. Rev. 2020 , 74 , 862–881. [ Google Scholar ] [ CrossRef ]
- Mykhalovskiy, E.; Hastings, C.; Comer, L.; Gruson-Wood, J.; Strang, M. Teaching Institutional Ethnography as an Alternative Sociology. In The Palgrave Handbook of Institutional Ethnography ; Luken, P., Vaughan, S., Eds.; Palgrave Macmillan: Cham, Switzerland, 2021; pp. 47–64. Available online: https://link.springer.com/chapter/10.1007/978-3-030-54222-1_4 (accessed on 23 August 2024).
- Walby, K. Institutional ethnography and data analysis: Making sense of data dialogues. Int. J. Soc. Res. Methodol. 2013 , 16 , 141–154. [ Google Scholar ] [ CrossRef ]
- DeVault, M.; McCoy, L. Institutional ethnography: Using interviews to investigate ruling relations. In Institutional Ethnography as Practice ; Smith, D., Ed.; Rowman & Littlefield Publishers: Lanham, MD, USA, 2006; pp. 15–44. [ Google Scholar ]
- Kearney, G.P.; Corman, M.K.; Hart, N.D.; Johnston, J.L.; Gormley, G.J. Why institutional ethnography? Why now? Institutional ethnography in health professions education. Perspect. Med. Educ. 2019 , 8 , 17–24. [ Google Scholar ] [ CrossRef ]
- Devault, M.L. Introduction: What is Institutional Ethnography? Soc. Probl. 2006 , 53 , 294–298. [ Google Scholar ] [ CrossRef ]
- Smith, D. Introduction. In Institutional Ethnography as Practice ; Smith, D., Ed.; Rowman & Littlefield Publishers: Lanham, MD, USA, 2006; pp. 1–12. [ Google Scholar ]
- Smith, D. Institutional Ethnography. Edited by Maria Xenitidou and Nigel Gilbert. Innovations in Social Science Research Methods. University of Surrey. January 2009. Available online: https://eprints.ncrm.ac.uk/id/eprint/804/1/ISSRM_Report_Public.pdf (accessed on 30 July 2024).
- Taber, N. Institutional ethnography, autoethnography, and narrative: An argument for incorporating multiple methodologies. Qual. Res. 2010 , 10 , 5–25. [ Google Scholar ] [ CrossRef ]
- Workman, E. Centering positionality in lifespan writing research through institutional and auto/ethnographic methodologies. In Improvisations: Methods and Methodologies in Lifespan Writing Research ; Dippre, R., Phillips, T., Eds.; The WAC Clearinghouse & University Press of Colorado: Denver, CO, USA, 2024. [ Google Scholar ] [ CrossRef ]
- Murray, J.; Swennen, A.; Kosnik, C. International Research, Policy and Practice in Teacher Education ; Springer Nature: Cham, Switzerland, 2019. [ Google Scholar ]
- Shaked, H. Instructional leadership in higher education: The case of Israel. High. Educ. Q. 2020 , 75 , 212–226. [ Google Scholar ] [ CrossRef ]
- Svend, B.; Kvale, S. InterViews: Learning the Craft of Qualitative Research Interviewing , 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2014; Available online: https://us.sagepub.com/en-us/nam/interviews/book239402 (accessed on 23 May 2020).
- Dhillon, J.K.; Thomas, N. Ethics of engagement and insider-outsider perspectives: Issues and dilemmas in cross-cultural interpretation. Int. J. Res. Method Educ. 2018 , 42 , 442–453. [ Google Scholar ] [ CrossRef ]
- Riger, S.; Sigurvinsdottir, R. Thematic Analysis. In Handbook of Methodological Approaches to Community-Based Research: Qualitative, Quantitative, and Mixed Methods ; Jason, L., Glenwick, D., Eds.; Oxford University Press: New York, NY, USA, 2016; pp. 33–42. Available online: https://global.oup.com/academic/product/handbook-of-methodological-approaches-to-community-based-research-9780190243654?cc=il&lang=en& (accessed on 31 March 2024).
- Mercer, J. The Challenges of Insider Research in Educational Institutions: Wielding a Double-Edged Sword and Resolving Delicate Dilemmas. Oxf. Rev. Educ. 2007 , 33 , 1–17. [ Google Scholar ] [ CrossRef ]
- Etherington, K. Becoming a Reflexive Researcher: Using Our Selves in Research ; Jessica Kingsley Publishers: London, UK, 2004. [ Google Scholar ]
- Lahman, M.K.E.; Thomas, R.; Teman, E.D. A Good Name: Pseudonyms in Research. Qual. Inq. 2022 , 29 , 678–685. [ Google Scholar ] [ CrossRef ]
- Lewis, M.J.; Quinnell, R. Telling tales out of school: Considerations of ‘insider’ research in higher education. Teach. High. Educ. 2024 , 1–13. [ Google Scholar ] [ CrossRef ]
- Czerniawski, G.; Gray, D.; MacPhail, A.; Bain, Y.; Conway, P.; Guberman, A. The professional learning needs and priorities of higher-education-based teacher educators in England, Ireland and Scotland. J. Educ. Teach. Int. Res. Pedagog. 2018 , 44 , 133–148. [ Google Scholar ] [ CrossRef ]
- Garry, P.M. Threats to academic freedom in higher education. Society 2023 , 60 , 176–180. [ Google Scholar ] [ CrossRef ]
- Levin, J.; Martin, M.; Damián, A.L. University Management, the Academic Profession, and Neoliberalism ; University of New York Press: Albany, NY, USA, 2020; Available online: https://sunypress.edu/Books/U/University-Management-the-Academic-Profession-and-Neoliberalism (accessed on 27 August 2024).
- Edwards, R. Why do academics do unfunded research? Resistance, compliance and identity in the UK neo-liberal university. Stud. High. Educ. 2022 , 47 , 904–914. [ Google Scholar ] [ CrossRef ]
- Resch, K.; Schrittesser, I.; Knapp, M.; Tedknapp, M. Overcoming the theory-practice divide in teacher education with the ‘Partner School Programme’. A conceptual mapping. Eur. J. Teach. Educ. 2022 , 47 , 564–580. [ Google Scholar ] [ CrossRef ]
- Liang, L.-F.; Lin, Y.-H. The struggle for ‘survival’ in contemporary higher education: The lived experiences of junior academics in Taiwan. In The Palgrave Handbook of Institutional Ethnography ; Luken, P., Vaughan, S., Eds.; Palgrave Macmillan: Cham, Switzerland, 2021; pp. 259–279. [ Google Scholar ] [ CrossRef ]
- O’connor, P. Is gendered power irrelevant in higher educational institutions? Understanding the persistence of gender inequality. Interdiscip. Sci. Rev. 2023 , 48 , 669–686. [ Google Scholar ] [ CrossRef ]
- Carr, M.; Clarkin-Phillips, J.; Earl, K.; Edwards, F.; Ferrier-Kerr, J. Writing group commitment and caring: Teacher educators talk about identities and agency in the Third Space of a writing group. Teach. Dev. 2020 , 24 , 669–687. [ Google Scholar ] [ CrossRef ]
- Cassandra, N.; Fithriani, R.; Febriyanti, R.H.; Mukminin, A. Becoming scholarly writers through professional learning community: A phenomenological case study of Indonesian teacher-educators. LEARN J. Lang. Educ. Acquis. Res. Netw. 2024 , 17 , 8–29. [ Google Scholar ]
- Fuller, R.; Brown, M.K.; Smith, K. (Eds.) Adjunct Faculty Voices: Cultivating Professional Development and Community at the Front Lines of Higher Education , 1st ed.; Stylus Publishing: Sterling, VA, USA, 2017; Available online: https://www.routledge.com/Adjunct-Faculty-Voices-Cultivating-Professional-Development-and-Community-at-the-Front-Lines-of-Higher-Education/Fuller-KendallBrown-Smith/p/book/9781620363720?srsltid=AfmBOoq-wPZOj-T9xPXwhQtjTS1uqpFhzqkJUfIHKG0v2r4vnYJH4O_F (accessed on 27 August 2024).
- Whitton, J.; Parr, G.; Choate, J. Developing the education research capability of education-focused academics: Building skills, identities and communities. High. Educ. Res. Dev. 2021 , 41 , 2122–2136. [ Google Scholar ] [ CrossRef ]
- Degn, L.; Franssen, T.; Sørensen, M.P.; de Rijcke, S. Research groups as communities of practice—A case study of four high-performing research groups. High. Educ. 2017 , 76 , 231–246. [ Google Scholar ] [ CrossRef ]
- Lave, J.; Wenger, E. Situated Learning: Legitimate Peripheral Participation ; Cambridge University Press: Cambridge, UK, 1991. [ Google Scholar ]
- Crompton, H.; Burke, D. Artificial intelligence in higher education: The state of the field. Int. J. Educ. Technol. High. Educ. 2023 , 20 , 22. [ Google Scholar ] [ CrossRef ]
Click here to enlarge figure
| The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
Share and Cite
Aharonian, N.; Schatz Oppenheimer, O. ‘If You Do Not Write, You Dry Up’: Tensions in Teacher Educator Research and Academic Writing. Educ. Sci. 2024 , 14 , 972. https://doi.org/10.3390/educsci14090972
Aharonian N, Schatz Oppenheimer O. ‘If You Do Not Write, You Dry Up’: Tensions in Teacher Educator Research and Academic Writing. Education Sciences . 2024; 14(9):972. https://doi.org/10.3390/educsci14090972
Aharonian, Nikki, and Orna Schatz Oppenheimer. 2024. "‘If You Do Not Write, You Dry Up’: Tensions in Teacher Educator Research and Academic Writing" Education Sciences 14, no. 9: 972. https://doi.org/10.3390/educsci14090972
Article Metrics
Further information, mdpi initiatives, follow mdpi.
Subscribe to receive issue release notifications and newsletters from MDPI journals
Narratives of Personal Health and Sexual Education Experiences of Emerging Adults with Disabilities
- Original Paper
- Open access
- Published: 02 September 2024
Cite this article
You have full access to this open access article

- Madelyn Toman ORCID: orcid.org/0009-0003-1021-0597 1 ,
- Rose Wesche 1 &
- Carolyn M. Shivers 2
Disabled communities’ sexualities have been historically oppressed. Currently in the U.S., public school curricula do not include inclusive sexual education and students with disabilities are often left out of classrooms that discuss any amount of personal health and sexual education (PHSE). Research on the disabled population is filled with samples of non-disabled individuals imposing their opinions on a population that they do not belong to. The purpose of this study was to capture lived experiences of ways emerging adults with disabilities learned about PHSE. Individuals with varied disabilities were intentionally included to add breadth to the research field. The final sample consisted of eight individuals (75% female, 87% White, mean age of 21.5). After conducting narrative interviews and analyses, four story types were generated: (1) “The Self-Guided Journey”, (2) “Experience is the Best Teacher”, (3) “Personal Health Matters More”, and (4) “Two Ears, One Mouth”. Our findings highlighted the lack of formal support and access to adequate, relevant information about sexuality for disabled communities. Informal sources, like families and media, sometimes served as helpful resources for PHSE and disabilities. Individuals’ disability symptoms and personal characteristics need to be considered when crafting universally applicable personal health and sexuality education.
Explore related subjects
- Artificial Intelligence
- Medical Ethics
Avoid common mistakes on your manuscript.
Introduction
Disabled voices are frequently missing from research about how to meet the needs of disabled people [ 60 , 65 ]. The exclusion of disabled voices from research on personal health and sexual education (PHSE) is a source of oppression, which can lead to nondisabled views, biases, values, and opinions being pushed on this population ineffectively and/or harmfully [ 52 ]. While research on PHSE for disabled individuals exists, very few of these studies—if any—include what disabled communities actually want and are not receiving [ 3 , 63 , 64 ]. Reducing sexual health disparities in disabled populations necessitates listening to what people with diverse disabilities say they need in their PHSE experiences. Footnote 1
Theoretical Framing
Multiple theoretical perspectives can inform research on PHSE among adolescents with disabilities. In this manuscript, we utilize theories on disability and sexuality that highlight the liberation of people with disabilities and their right to experience consensual, fulfilling, and pleasurable sexual relationships. These theories include the widely-accepted social model of disabilities [ 8 , 56 ], crip theory of sexuality [ 46 ], and the normative framework of sexuality development [ 62 ].
The social model of disabilities offers a general guiding framework of appropriate ways to view disabilities in context. This widely accepted model challenges medical models’ view of disabilities as internal deficits. According to the social model, societies create barriers that everyone encounters daily though not every body can overcome. Disabilities affect people’s functioning because of environmental, social, and economic barriers [ 8 , 56 ]. Crip theory of sexuality also considers how society can empower or disempower people with disabilities. As a branch of crip theory [ 45 ], McRuer’s crip theory of sexuality ([ 46 ] considers (and reconsiders disabled peoples’ rights and pleasures, while including how they may be assisted by the state/legislative bodies (to the desire of the disabled community,[ 46 ]. The social model of disabilities and crip theory of sexuality’s emphasis on rights and pleasures of individuals with disabilities serves as a guide to analyze and represent the community in a humanized, enlightened way. Disabled people are not inherently less sexual or less able to participate in sexual activities, rather, a lack of inclusive and comprehensive PHSE resources puts them at a disadvantage.
The normative framework of sexuality development [ 62 ] proposes that sexuality development is a normal, expected, and necessary part of adolescent development. Under this framework, the term “sexuality” includes multiple behavioral and cognitive domains, such as sexual behaviors, safer sex, sexual identity, and attitudes toward sexuality. Previous research has used the normative framework of sexuality development to investigate aspects of sexuality development with disabled adolescents [ 14 ], though there needs to be more incorporation of this framework with disabilities studies.
As we understand and make sense of these three theories, the research team used each of the theories as a lens to frame our analyses and interpret the bigger picture within the study. Research that is theory-informed and influenced by the opinions of the community it serves (i.e., the disabled communities) can assist in eliminating harmful structural practices. Alienation, stigmatization, and discrimination are all ways that societal systems attempt to extinguish sexuality for the disabled population [ 9 ]. Ableist views embedded in policies, laws, and supports harm the disabled community they set out to serve. A direct result of ableist influences is internalized ableism, which is the projection of negative ableist feelings onto people with disabilities who then internalize and believe them to be true [ 34 ]. Internalized ableism can be incredibly damaging to disabled individuals. The research team intentionally incorporated theory from disability studies and the experiences of disabled individuals to reject ableist views and biases.
The Current State of PHSE for Disabled Communities
Misperceptions of people with disabilities' sexuality have been a common reason for not providing the population with sexual knowledge. This population is often incorrectly thought of as asexual, having no sexual feelings or desires [ 5 , 47 ]. Additionally, people with disabilities are often thought of as needing protection [ 47 ]. Perhaps as a result of these misperceptions, policies related to education and sexuality neglect the needs of people with disabilities. The Individuals with Disabilities Education Act (IDEA) (2004), which provides all individuals with disabilities a right to free, appropriate public education that is tailored to their needs, does not require schools to teach disabled students about sexuality. This omission, coupled with often inadequate sexual education in U.S. middle and high schools, means that students with disabilities are often not included in sexual education classes [ 55 ]. Consistent with crip theory of sexuality’s emphasis on rights and autonomy, the exclusion of people with disabilities from sex education is another way that society fails to consider the sexual rights of the population.
Previous research has shown that young disabled communities’ needs of sexuality and health education are not being met [ 40 ]. For example, a pilot study implementing sex education for young intellectually disabled individuals found that what would be most helpful for the young intellectually disabled population is an adapted model for PHSE that is consistent with varying individual circumstances [ 40 ]. When sex education needs are met, individuals with disabilities experience increased knowledge of personal and sexual health [ 30 ].
In the absence of school-based PHSE, adolescents with disabilities may rely on family members and community programs to learn about health and sexuality. Families and caregivers of people with disabilities typically acknowledge that their care-recipient should have some sexual knowledge, though they do not know the best ways to teach it [ 24 ]. Gray and colleagues found that even though children with cerebral palsy were at risk for abuse, with families frequently discounting the likelihood of abuse due to the child’s disability. Since not all family members know how to educate youth about PHSE, some resources, like conversation models and question guides, have been created to assist with such conversations [ 10 ].
Consequences of Inadequate PHSE
As a direct consequence of not receiving effective PHSE, people with disabilities are made more vulnerable to negative sexual health outcomes. The risk of victimization and sexually transmitted infections is significantly higher for men and women with disabilities than nondisabled people across their lifespans [ 6 , 27 , 41 , 42 ]. These risks are related to a lack of PHSE. People with disabilities sometimes have less knowledge of what is happening to their bodies and how to protect themselves and others because they are not taught appropriate PHSE [ 38 ]. This lack of knowledge makes them vulnerable to abuse. People with disabilities also may not know how to protect themselves from things like STIs/STDs and pregnancy during consensual sexual activities [ 41 ]. Access to proper healthcare is also much more challenging for adults with disabilities—another way that society places barriers on sexual rights of the population [ 25 ]. So, even if equipped with knowledge, accessing the required materials to prevent unwanted outcomes of sex is difficult.
Barriers to PHSE for Disabled Communities
Even though there has been some headway made for improving PHSE targeted for disabled communities, current research has only provided limited insights into the PHSE needs of people with disabilities. One barrier to addressing disability and sexuality is limited use of disabled voices in research and policy. Research on disability and PHSE targets parents and clinicians, while young disabled individuals are not used as active participants in research covering their own population [ 17 , 37 , 60 , 65 ]. As a direct result, inexperienced and ableist ideas are inserted into regulations and supports for the disabled population. Family members, clinicians, and caretakers have become the voices and experts of the community. Centering the voices of caregivers and providers takes out the involvement of disabled individuals altogether. Although it is important to provide caretakers with supportive guides to assist in caregiving, resources should be made for individuals with disabilities and serve as supportive tools for aids and caretakers. Using disabled individuals as participants in studies about disability will lead to proper representation.
Another barrier to more expansive research combining disability and sexuality is the tendency to target populations with singular, specific types of disabilities. In their literature review of available PHSE resources for people with disabilities, Treacy and colleagues [ 63 ] provided a useful table with various books and sources to use as educational tools for families and individuals with specific disabilities. Researchers have investigated the ways people with intellectual disabilities may effectively learn about PHSE topics [ 30 , 40 , 54 ],the fertility/infertility, sexual health, and prevalence of STIs/STDs among people living with cystic fibrosis [ 7 , 16 , 21 , 29 ],and the education and sexuality of people with Down Syndrome [ 4 , 10 , 23 , 43 ]. This research on specific disabilities has provided depth of understanding of these areas. However, focusing research on a few specific types of disabled individuals leaves room for the assumption that findings can apply to all disabled communities. Disabilities are diverse, and the disabled community is not monolithic. What is appropriate for individuals with invisible disabilities may not serve individuals with visible disabilities or individuals with co-occurring disabilities. By including people with multiple types of disabilities in a study, researchers can gain more understanding of diverse lived experiences of various disabled communities. This breadth of understanding is necessary to create curricula that can meet the unique and overlapping needs of people with diverse disabilities.
The Present Research
PHSE is vitally important because everyone—regardless of “ability”—goes through biological changes, like puberty, that impact their day-to-day actions, interactions, feelings, thoughts, and desires. The goal of the present research was to understand the PHSE experiences of emerging adults with disabilities. Personal stories of the lived experiences of PHSE not only tell us what is being taught, but how this information is being communicated and how effective it is. Retrospective narratives gave insight to the perception of PHSE from people living with disabilities based on how stories were told, thus providing more information about the strengths and gaps of PHSE and the needs of adolescents with disabilities. We used a narrative, qualitative approach to honor the experiences of people with disabilities and center their voices while empowering them and promoting an inclusive, accurate representation of PHSE [ 22 , 28 , 59 ]. We intentionally sampled participants with multiple types of disabilities and symptoms to represent unique and shared experiences of PHSE and sexuality development across the disabled population. The results of this study add breadth to the research field.
Research Question 1: How do emerging adults with various types of disabilities experience personal health and sexual education?
Research Question 2: What do the stories of emerging adults with various disabilities suggest about their satisfaction with their experiences of PHSE?
Recruitment
Recruitment took place between August 2022 and February 2023. Participants were recruited through advertisements and word of mouth in and around two towns home to college campuses. Advertisements and announcements were also made in classes related to sexuality and/or disability. Inclusion criteria required participants to be between ages 18 and 24 and have at least one diagnosed disability from a medical professional. People with intellectual disabilities were not included in the sample because of logistical barriers to obtaining consent and because recruitment efforts focused on college campuses, where people with intellectual disabilities do not frequently attend.
Participants
When working with vulnerable, previously exploited communities, it is vital to consider the best ways research can support participants [ 50 , 58 ]. Narrative research methods in disabilities studies empower individuals with disabilities and promote inclusive, accurate representation [ 22 , 59 ]. Accurately representing lived experiences was accomplished through open-ended and participant-led conversations, summarizing information with participants during interviews so they could correct possible misinterpretations, and reflexive work by the primary investigator to consciously keep preconceptions out of data. In this way, participants were involved in research collection and analysis. Privacy was maintained through deidentification of transcripts and correspondences.
Eight participants completed semi-structured narrative interviews over Zoom. Narrative methodological studies typically have lower sample sizes to show the depth of a few individuals’ experiences [ 33 ]. Participants’ mean age was 21.5 (range 18–25). The sample included six women, one man, and one person who identified as non-binary. A large majority of the sample was Caucasian ( n = 7) and one participant was Black/African American. Not all participants disclosed their sexual identities ( n = 4), but of those who did: one identified as bisexual, two identified as heterosexual, and one identified as queer. All participants were students; three participants were graduate students and five were undergraduate students. Four participants described receiving at least one diagnosis prior to high school, and all eight participants received at least one of their diagnoses by the end of high school. Three participants described having in-school accommodations from elementary to high school, specifically IEPs and 504 s, and no participants experienced self-contained classes or being placed in Special Education tracks. The following are all of the disabilities that participants identified with: type one diabetes ( n = 2), bilaterally deaf ( n = 1), hearing impaired/partial deafness ( n = 1), Attention Deficit/Hyperactivity Disorder ( n = 5), Generalized Anxiety Disorder ( n = 2), Obsessive Compulsive Disorder ( n = 1), Crohn’s disease ( n = 1), autistic ( n = 1), disordered eating ( n = 1), thyroid disease ( n = 1), a herpes diagnosis ( n = 1), and acquired neurological disabilities ( n = 1). Several participants had comorbid disabilities, so no disability listed was mutually exclusive. Participants described acquiring disabilities and/or receiving diagnoses at different stages during development from childhood to their current stage, emerging adulthood. Although some of the disabilities were acquired after school-based PHSE, participants discussed a range of disabilities that were relevant to their PHSE experiences.
Individuals interested in the study contacted the primary investigator through email. Once eligibility was determined, each participant engaged in a virtual semi-structured interview on the Zoom platform. All interviews were audio recorded, and consent was obtained before proceeding with protocol questions. The procedures and protocol for this study were approved by the Institutional Review Board at Virginia Polytechnic Institute and State University.
Each interview followed a narrative methodological structure. Participants were asked to begin by explaining their personal meaning of sex education (“When I say sex education, what do you think of?”). Then, they were asked to tell the story of how they learned about personal health and sexuality development (“I want you to think of your journey with PHSE as a story with characters and plotlines, etc. Whenever you are ready, please share your story with me.”) Once the participant finished their narrative, the interviewer asked probing questions that were dependent on the story each participant told. In order to provide more detail, participants responded to questions about their perceptions of experiences, the influential characters that they mentioned, turning points in their story, and their overall satisfaction with their PHSE journeys. The interviewer asked clarifying and interpretive questions during interviews to ensure accurate interpretation of participant experiences.
Data Analysis
After the interview was complete, the interviewer transferred the audio recordings to a university secure virtual location. All interviews were transcribed verbatim using audio recordings and de-identified them for participants’ privacy. Recordings, transcripts, and memo files were also labeled with ID numbers and aliases.
The research team analyzed the raw interviews using thematic narrative analysis [ 51 ]. Thematic narrative analysis focuses on the content of participants’ stories, deconstructs each narrative during analysis and thematic generation in order to identify core narratives, and then reconstructs segmented stories to present narratives as they were told. The goals of this method are to preserve the essence of participants’ stories, focus on what is being said (vs. how or to whom), and to identify the core of each narrative or story types being told. At the end of analyses, story types present the different ways participants experienced the phenomena and help situate individual narratives in relation to other participants’ [ 33 ]. The goal for analyses was to first identify themes and then construct story types that reflected the themes in the data.
Story types were essential to the study because stories are powerful. Stories are ways of synthesizing information. People make sense of their experiences through memories and recounts of their stories. Therefore, the type of stories that are shared when describing PHSE reflect memorable, unique experiences. A person’s disability adds a layer of context around their story as it affects how they interact with others, their environment, and sometimes themselves.
All eight interview transcripts went through sequential readings (guided by [ 33 ]), which is traditional in narrative analysis, for familiarization. The primary investigator, who conducted each interview, was also the primary coder for each transcript. For this study, the first three rounds of coding focused exclusively on content of the narrative and identifying themes. Initial codes were based on thematic content and the overall structure or pattern of the narrative (example codes: “PHSE not present in school”; “Failure/Distrust of Medical Providers”; “Self-led Journey”). The investigators used initial codes to define themes throughout each transcript, which led to segmentation within the data. Then, the following two read throughs focused more on key voices, characters, and important influences within the narrative (example codes: “Peer Pressure”, “Messages from Parents”; “Media was a PHSE tool”). Once the primary investigator generated a codebook comprised of each transcript’s themes, the investigators identified similarities or links between transcripts and began generating story types. At this point during analysis, the investigators unsegmented transcripts, or restructured narratives to their original forms, to preserve the context of codes [ 51 ].
The primary investigator kept memos during the analysis that reflected on their position in the data as well as thoughts, feelings, and observations. A co-investigator assisted in the latter half of analyses to offer additional insights and interpretation of the data. Together, the investigators discussed, debated, and ultimately collaborated on story type construction based on themes found in the data. Across the eight narratives, the research team constructed four story types based on shared or unique experiences, similarities, and differences in experiences across the eight participants.
Positionality
The investigators for this study have diverse, unique, and overlapping social identities and academic training and appointments. The research team has expertise in developmental research, disability studies, and qualitative research. We recognize some of our in-group memberships for this study as well as our potential biases and similar lived experiences. The principal investigator, who led each interview and the analyses, has acquired disabilities and disclosed her diagnoses to each participant during their interview. In order to preserve the narratives of our participants and co-constructed findings, reflexive practices, like memoing, and multiple team discussions during analysis assisted in honoring the lived experiences of our participants and truth within their narratives.
Using thematic methods for narrative analysis, four story types were discovered from the stories of the eight participants: (1) “The Self-Guided Journey”, (2) “Experience is the Best Teacher”, (3) “Personal Health Matters More”, and (4) “Two Ears, One Mouth”. Each story type held combinations of unique experiences of participants and shared experiences across participants. Below, each story type is described along with the role of disabilities and sources of sexual information (or lack of information), like schools, families, and medical providers. Table 1 shows participant pseudonyms and story types with supportive themes.
The Self-Guided Journey
As the name of this story type implies, the three participants that experienced “The Self-Guided Journey” actively educated themselves on personal health and sexual topics after not receiving the information they needed from authority figures. Although some participants described PHSE resources that attempted to educate them and some resources that failed to provide accurate support, all three participants who described this story type needed to find their own communities and educational resources in order to accumulate all of the PHSE information they needed. One key characteristic of this story type that was different compared to other narratives was that each participant emerged as the main character in their story—they were actively involved in every step of their PHSE journey.
Interestingly, each participant who described this story type was diagnosed with a disability after childhood. Most of the sex education that they discussed took place before their disabilities were recognized/diagnosed. Another characteristic of these participants’ narratives was that their disability symptoms were woven throughout their entire narrative. All three had clear reflections about how their disabilities impacted their personal health, romantic relationships, and sexual lives.
Failure of Formal School PHSE and School Support
Public school PHSE was unhelpful and fear-based for these participants. The curriculum they experienced was neither inclusive nor comprehensive.
[Sex education in school] wasn't very inclusive. I want to say they really only teach you how a woman can get pregnant. And basically, that's it, the sex, organs and reproductive system. Sometimes he would go into a little bit of detail like when a woman can get pregnant, they can still get pregnant during their period. And that's basically it… thinking back on it, you realize that it was mainly two gendered males and females that you're always thinking about. And they never talk about the emotional aspects of it either. And there was literally no discussion at all as far as disability. (Stacy)
Brandy reflected on how school sex education failed to give her social and communication skills that would have helped in relationships later in her life.
I realized that sex ed in high school does a lot of fear stuff. So, I felt very afraid of a lot of STIs. But one thing that I lacked was the ability to communicate, especially with people I was hooking up with, about my boundaries … I think [my struggle with communicating to sexual partners] is a combination of not being explicitly taught self-advocacy in childhood and kind of struggling with that in general. I'm a certified people-pleaser, so that you know just all of those things together I think, really came together to influence some not so great decision-making on my part.
Jude echoed the other two participants in their desire for more comprehensive, inclusive sex education in public school. Jude added how the exclusion of non-heterosexual information left them without key information that would have been helpful given that they are queer and non-binary. Aside from PHSE, Jude’s school system stopped providing physical accommodations and support once their acquired disabilities became less visible:
[There was] absolutely no queer representation or no disability representation at all [in school sex education]. I think everyone at least in my class did not have a physical disability that was visible or apparent. So, it just wasn't at the forefront of anyone's mind… People were really good when I had these physical indicators of injury, but once those physical indicators were gone, like I still have- I developed a neurogenic stutter... and my memory was still pretty awful, and I could do assignments but I needed more time. But I could do all the things, and thankfully a lot of it came back, but once the physical indicators were gone, it was like ‘Oh, Jude's healed, like Jude's fine’ when I was not fine by any stretch of the imagination. So yeah, it was this really weird mix of like physical indication versus invisible disability plus not wanting us to sue the school system [for the injuries] and my mom being a special education teacher and trying to keep me on track. So, it was a lot all wrapped up together, which, like, had some very interesting implications for, like, how people handled everything … like, once all the physical indications of disability were gone [the accommodations were gone too].
Mixed Parental Guidance
Although Stacy, Jude, and Brandy had similar feelings about their school-based sexual education, they had different experiences with family sexual socialization. Stacy’s parents were caring and held opinions about dating or sexual behaviors, but they did not communicate or converse about PHSE topics with her. There was no conversation even when she experienced concerning changes in her menstrual cycle.
I did not learn much from my family. My dad tries to tell me about how emotionally I should only deal with people who make you feel good and things like that. But, like, to have [a sex] conversation with my dad, just is like- it just didn't happen… And then my mother, she's funny too, like we just don't talk about it. But there was an incident where I was, like, seeing a boy and I was about 17 and it was a hard, toxic situation. So toxic that, like, I had skipped my period for a whole month and we weren't having sex or anything like that. But it was close to the point where [my mom] felt like, ‘Oh, you haven't had your period.’ Like, I had gone to the nurse and then she told me that I should tell my mother. So, I told her and she was so upset with me. And we went to the gynecologist and she put me on the pill. That was literally the whole thing… And so, it was a really scary and hard situation, but me and my mother, we didn't really talk much about it at all. She just put me on birth control and then that was it. Yeah. So, my parents did not really give me a lot of sex education.
Brandy’s parents did not have conversations about sexuality, but they provided resources for her to learn from and safer sex mechanisms, like condoms and birth control, when she needed them:
I remember, my parents are very passive people, and my sex ed at home consisted of coming home from school one day, and I found, like, three books on my bed about sex. They were great. They were really good resources, I think one of them was published by the American Pediatrics Association. One of them was more informal, and had, like, illustrations in it, and I don't remember what the other one was, but it was pretty much understood that I could ask any questions that I needed to, but my parents didn't want to start the conversation… I got the depo shot and then started dating my high school boyfriend, who I later had sex with. I remember my mom found condoms in my dresser, and she was like, "Hey, just wanted you to know I know you've had sex. We don't need to talk about it," and I was like, "Great."
In contrast to Stacy and Brandy’s lack of communication from parents about sex, Jude had an open, communicative relationship with their mother when it came to personal health and sexuality. Their mother grew up with no PHSE communication in her family, so she made the active choice to be open with Jude when they were ready to have those discussions.
My mom was always very good about having those conversations, if and when I needed them, or when I had questions she answered them. I don't really remember what those questions were, but she was always very receptive and happy to answer them in developmentally appropriate ways.
Feeling Separate from Peers
Although this was not a part of Stacy’s PHSE story, both Jude and Brandy felt separated from their peers because of disability-related health outcomes. Brandy explained how delayed puberty was a symptom of her Crohn’s disease, so when her friends’ bodies were changing and they were becoming interested in dating and romantic relationships, she felt behind:
I was undiagnosed for so long. I had an extremely delayed puberty, and I think that that was a huge influence on my sex education, because I felt very behind all of my peers. Throughout high school especially [I felt behind because] I didn't get my period until I was 16, and that was a time where I started hearing sex talked about more around me. So, there is kind of like that disjointedness, I guess, where I was dealing with all of these health things and it was causing my puberty to be delayed. I felt like crap all the time. Just no energy. I couldn't really keep any nutrients down. And then all my peers were talking about sex like it was this fun thing, you know, and I was just, like, I don't see anywhere that fits in my life just because of all the issues I was dealing with, so that that I think is really important when it comes to my journey with all of that is just being very physically behind my peers developmentally.
Jude experienced almost the opposite when they went through puberty before their peers. Although their puberty was not related to any diagnosis, early breast development led to being sexualized by peers, particularly boys, and Jude turned towards their hyperfixation on academic achievement to mediate anxiety. Jude self-identified as autistic and having ADHD and explained how “it was kind of like the chicken or the egg thing”: hyperfixation on school work helped ease the anxiety about sexuality development and peer treatment, but their sexuality development and academic success caused unwanted peer treatment that led to anxiety.
The sexualization that came from like little teenage boys who thought that they were being funny and made the comments around like, “Oh, did you get a boob job?” I think at that point in time academic validation became that much more important because I wanted to be seen as more than just like my body, which I think is really interesting… It was an awful cycle of being perceived as like a woman in a way that was very restrictive and made me want to achieve highly, but I was already achieving highly. So it was just like this awful circle, until, like I broke like, and I never felt comfortable with how people were perceiving me from a gender perspective.
Jude and Brandy demonstrated connections between disability and sexuality development in different ways, illustrating the bidirectional links between these processes. Sexuality development can be influenced by disability symptoms, as Brandy discussed, just as disability symptoms can be influenced by one’s sexuality development experiences, as Jude discussed. The interaction between disability characteristics was also apparent in the second story type, “Experience is the Best Teacher,” that is described below.
Failure of Medical Providers
All three participants described various failures of medical providers, specifically doctors and nurses. Each had doctors that provided unclear or incorrect information regarding their diagnoses and how their sexual or health related circumstances may be affected. Participants’ inadequate healthcare experiences for sexuality were also tied to inadequate healthcare broadly. For example, Stacy explained how her journey with birth control began with a doctor providing her with a “one–size-fits-all” advice model that was not actually helpful in reality for people living with diabetes:
Like with the Depo shot, I noticed that I had to use a lot of insulin…If I want to get back on some kind of birth control, I would have to do the trial and error and just see what's right for me. As far as [doctor name], my OB-GYN, she was telling me the shot is like the best thing for a diabetic and it's amazing. It's like it's a one size fits all or something like that. She was basically telling me I should have been able to perfectly live with the Depo shot. And that was not correct at all because my blood sugar was so high for the longest time, and I realized that it was [because of] the depo and I had to wait three months for it to get out of my system. And so yeah, a lot of things where- a lot of these doctors they think it's like a one size fits all for everything that comes with diabetes and even the nurses when I felt like my feet were hurting or tingling, she would tell me, “Oh, that's not like that's weird.” That's not something that I've ever heard of before. But I've talked to other diabetics and they're like, “Oh yeah, like you might want to make sure you're doing better, like you're keeping up with your insulin because that could be the start of neuropathy in your hands and feet.” And so yeah. Like when you ask those kinds of questions, they think they just give you an answer that they gave everyone else, but it just does not work that way… I feel like in health care settings, it's a little cut and dry. They tell you what they tell you in bulk. They told me to stay away from pastry, stay away from all this stuff only on good occasions, like happy occasions when you want to eat things like that. And so, when I actually looked up, there was like Beyond Type One that's like a website for type one diabetes like Nick Jonas was like a part of it or something like that. And so, I did learn a lot from it. However, it was like a source that I didn't find from an actual doctor.
Unhelpful information from doctors about sexual health mirrored dissatisfying medical experiences about disabilities. Jude experienced misdiagnoses that led to not receiving helpful treatment options.
I was very, very anxious. So, I was on anti-anxiety [medication]. In hindsight, it was like a lot of it was probably ADHD that was terribly misdiagnosed. They also almost misdiagnosed me with borderline personality disorder, because I was describing kind of like… more or less the highs and lows of ADHD, where it's like I super hyper focus and I don't have any energy. And they didn't ask good enough probing questions to get at any of it, cause like I had great grades like despite all these injuries, I still had A's and B's, and as a child, I was a perfectionist like very stereotypical, like female presenting ADHD that no one caught, because that's not how we perceive like ADHD in children because all the studies are based off of like small boys. So, the medication helped a lot with my anxiety that came alongside ADHD, but I still was always kind of like, I have this little bit of anxiety, because I wasn't actually being treated with what I needed to be treated for.
Brandy explained her “pattern of distrust of doctors” throughout her interview. This distrust began in her adolescence when she questioned how her diagnosis of Crohn's disease would affect her ability to have children and her doctor responded: “Why are you thinking about having kids right now? You’re in high school.” Then, when she went on birth control, her nurses did “everything in their power to make it the worst experience possible”.
Interviewer: What do you mean in their power? Brandy: So, my doctor prescribed it, but it was always the nurses that would administer the shot. And they would do things, so I would go by myself to get the shot without my parents, and that was just kind of at a convenience, not because I didn't want them there. I would go, and the nurses would use the largest needle possible. I didn't find out until I'd already been getting the shot for 2 years that it could go in my arm, and you didn't have to use, you know, a 16-gauge needle, which is a massive needle. They would require that I get the shot done in my thigh, so they made me get undressed in order to take this shot and they used a huge needle. Any time I requested to have the shot [then] a couple of days earlier or later than the exact date that was 3 months past the other one they'd make me take a pregnancy test, or they tell me I'd have to come back and do it another time. So, just things like that made the experience awful.
She hypothesized how the reactions of nurses and doctors could have been due to the southern United States cultural context, which she perceived as unwelcoming to sexually active young women. Whatever the reasoning, she confided that it felt like she “was being punished for needing something” which led her to stop raising questions to medical providers and seek answers herself.
Actively Seeking PHSE
Because teachers, family, and medical providers lacked PHSE information that was relevant to their lives, all three of these participants sought out their own answers to questions and sexual/health inquiries. Jude’s turning point (as described above) was when they realized that authority figures, specifically doctors and medical care providers, could not give them all of the information specific to their sexuality development. Brandy had the same pattern of distrust with medical care providers that solidified her inability to rely on them as sources of PHSE.
Similar to Jude and Brandy, Stacy explicitly connected her lack of PHSE in school and from doctors to her needing to find her own answers regarding sexuality and health. She described early in her narrative a time she asked a teacher about periods while in a sex education class and he had dismissed the question altogether. This experience started her on a path of not being able to discuss her sexuality development with authority figures. Stacy’s thoughtful reflection made her turning points, or narrative climaxes, that much clearer upon analysis.
As far as sex education, everything that I've learned, that I've known about, is something that I've had to learn on my own. It's not something that I've learned even like in [school] … Although I didn't learn that much about disability and sex education [growing up], what I have learned on my own has been pretty good. I tried to take everything one day at a time. I just do what I can and not think too much about what could happen if I don't take care of myself… My experience is that I do what I can with the information that I'm given because I seek out that information.
Finally, the internet was an educational tool in all three of these PHSE journeys. Jude discovered gender and sexuality information through YouTube videos and other internet platforms, which taught them about trans health, non-binary identities, and sexual activity options, like engaging in kink, for individuals with varying abilities.
I ended up consuming more and more information [on the internet about] like kink communities and like trans communities, and like different abilities, just like so I had all those tools in my toolbox, like, if someone ever were to need them. Sometimes they have been super necessary and helpful, and sometimes it's like, why, why do I know this thing? It's cool that I know this thing in case it ever comes up? But is it ever really gonna be necessary? Probably not. So, yeah. So, a lot of informal sex education existed for me… I was able to find a majority of what I needed in some way, shape, or form. I just had to get really, really creative about the avenues in which I searched for those things.
Stacy also found a helpful community online of people with her same diagnosis. They were able to give her advice about birth control options and outcomes, which her doctors proved to be unaware of.
I had to learn a lot of what I know about my disease through other people on Facebook and on Twitter. I found a really good community on Twitter about having diabetes…I found [useful sexual health information] from my type one diabetes groups. And so, they talked about different birth controls you can use as a type one diabetic.
Experience is the Best Teacher
Now, I think I'm very educated, but that came from experience and from asking questions that I didn't even know how to ask at the time when I was being educated. I didn't…like, nobody educated me enough to find the questions or know what questions to ask or know what questions were important. So, I think now, I mean, it's taken many years and sexual experiences to actually figure out how to navigate sexual relationships and just being smart and safe and stuff. (Amie)
In the second story type, three participants learned about sex and personal health through experiences with others, or vicariously through others, or after an experience happened and each participant raised questions. This is different from the “Self-Guided Journey” story type because participants were not actively seeking sexual knowledge in order to educate themselves. Additionally, where participants who experienced the “Self-Guided Journey” described themselves as the main characters of their story and having turning points where they took initiative in their sexual journeys, participants who described the “Experience is the Best Teacher” story type described being more passive within their stories, soaking in the things that happened to them and around them. Personal, shared, and others’ experiences served as “teaching”, or lessons on PHSE. Their friends, siblings, romantic partners, and media were important characters in their narratives. Alice’s reflection encapsulates the role of others in PHSE: “even though my school didn't teach me that much like the media and the people that I'm surrounded by taught me like a ton.”
For the participants who described this story type, their disabilities were woven into their stories, though not as apparent as those from “The Self-Guided Journey”. None of these participants highlighted their disabilities within their narratives during formal sex education. Rather, the influence of disabilities emerged towards the middle and end of their interviews when describing experiences that they later learned from. Describing their disabilities and symptoms near the end of interviews showed how participants who described this story type had not considered previously how their disabilities impacted their sexuality development; in contrast, in “The Self-Guided Journey”, participants had clear reflections on the intersection of disabilities and PHSE experiences. In this way, formal education was not nearly as helpful in their disability lives as lived experiences.
Unhelpful School Sex Education
If sex education was present in school, it was not sufficient to equip participants with the tools/social skills they needed. Formal education was conceptual and did not provide practical guidance for navigating the challenges of sexual and romantic relationships. Insufficient school PHSE was one way that the “Experience is the Best Teacher” story type was similar to “The Self-Guided Journey”.
One participant did not receive any school-based PHSE. Alice described how her class “got to the first day [of formal PHSE] when they were talking about the organs. And then our heater broke in our school and it was the end of the semester, so we just never finished the class.” Although Alice did not receive any formal PHSE, she hypothesized that it would have been abstinence-based:
I went to a Catholic middle school, so I'm pretty sure they would have not been like, “Go and do your thing, just be safe.” I'm pretty sure it's not what the Catholic Church then or I'm sure now is really preaching. I'm sure it would have been, “Hey, here’s all these things so you know about it, but you need to wait until marriage because that’s what’s expected of you.”
Early in her interview, Amie proposed that more comprehensive PHSE would have been helpful to her as she managed her disability:
I think a lot of people with ADHD and other disabilities might not have the social skills to adapt to, like, navigate that type of situation. . . And [what is being taught in school] I mean that's not really helpful when you have to figure out what to do in an awkward situation. I think that that's really important and that there should definitely be some education on that, especially for people who might struggle because I think anxiety sometimes causes me to just shut down when I'm in an extremely uncomfortable position. And just like maybe something I'd be able to do when I wasn't super anxious. I'd be able to navigate that situation, but if I'm super anxious about a situation, it becomes a lot harder to navigate my way through a situation.
Reactive Discussions with Family Members
Conversations with family members, particularly parents, occurred in response to sexual situations instead of proactive discussions before participants became sexually active. This contributed to the narrative of “Experience is the Best Teacher” as participants were having sexual or personal health related experiences before having discussions around what those experiences may be like. Amie, for example, described her first conversation with her mother about periods after she got her first period:
But anyways, so yeah, very little sex education at that point. Then once I got my period… I went and talked to her about it and she explained all of that and what to do with tampons and pads.
Then, Amie had a similar encounter with her mother after engaging in sexual activities:
Amie: I mean, like once I started having sex, and once my sister started then my mom- Like, sometimes my mom would just say to be safe. She put us on birth control and stuff. But yeah, not much. No. I mean, we didn't have conversations much about other things besides just, you know, be safe. Interviewer: Okay. And those conversations came up after- after you started having experiences? So, like your mom talked about periods after you got your period? Amie: Yes. Interviewer: And about sex after you've had sex? Amie: Yeah.
In another story, Gabrielle described indirect sexual communication with her parents and conversations after she became romantically involved:
In middle school, it was not like, ‘Alright, we're gonna sit down and we're going to have this [sex conversation].’ like my parents …they paid attention and care about what we're doing …The conversation of sex in general was indirect. Like when we were just talking or we'd be watching TV and it'd be like jokingly. My dad [would say] "That's what she said". Or like jokes like that. So, we understood the concept of it because of that.
Alice had similar, comfortable communication with her mother, but after having experienced dating and beginning sexual activities, like kissing and fondling:
I think around like my sort of figuring things out and freshman year in high school, I'm sure my mom and I were watching something and she's like, “Do you know how this works?” And I was like, “Yeah, but you can kind of give me the run?” and she gave me a very quick rundown on how it works, but it's a very quick thing just because… it was a very uncomfortable conversation to be having with my mom as a 14-year-old girl who was very new to the whole thing. Like she's been obviously more open about that now as I've done stuff [with my boyfriend].
Vicarious Learning
In addition to personal experiences, these participants learned about personal health and sexuality vicariously or socially from siblings and peers. Gabrielle spoke about not being “the sexual type” in high school and learning about dating once her friends were romantically involved:
I didn't really, like, [I wasn’t] the sexual type. Like I just didn't think about that. I was more focused on my schooling studies. I got a big group of friends and I had guy friends too, but it wasn't like a big deal to me. But then I guess around junior year is when I started getting interested in [romantic relationships], you know, because of my friends. I don't know if it was like peer pressure necessarily, but it was just like, ‘Okay, I'm getting older, like, I'm about to go to graduate.’ Like, I don't know. Like, I feel like just learning from others is what helped me the most understand how things work.
Similarly, Amie’s sister began dating before she did and her curiosity led her to raise questions:
Interviewer: And then so was she just, [your sister] was just around and you ask questions or- Amie: I feel like it was more of her telling me stories I didn't really need to know. But I had questions about those stories. Interviewer: So, hearing about her experiences? Amie: Yes. And then Just being curious. Like how does that work? Like what did you do? Like Are you pregnant? Like stuff like that.
Personal Experiences
Participants who described this story type had personal experiences that taught them about their sexuality overlapped with disability symptoms.
Relationships and sex “clicked” for Alice as she entered high school and her peer group began talking about sexual taboo topics more openly. Once she began dating, she experienced anxiety, panic attacks, and eventually developed an eating disorder. She had to then learn how to communicate and respond in sexual scenarios once her disability symptoms arose. One example Alice told was about a time when she was in a car with her boyfriend and he attempted to kiss her:
So, my system was just overstimulated and he was trying to make a move [to kiss me]. And I was just like, and I basically was like staring at his joystick and he was like, “Are you okay?” And I was like, “No you need to drive or distract me because I think I'm starting to get an anxiety attack.” So, if we’re driving and I didn't really know what was making me anxious because I was like, “Oh, maybe it's the ice cream or it's just this kid [trying to kiss me].” Then he was like, “Hey, am I the reason you're anxious? Like you're afraid to do anything physical with me.” And I was like, “Yes, honestly like I am because this is intimidating. I'm not even sure how I feel about all this. Like this is all happening very quickly.” Like he came over to my house and we hung out, made out and I was like, I don't really enjoy this. And I was like, if this is what kissing and making out is like, I thought this was supposed to be nice and magical and I'm not feeling that at all.
Amie reflected on how her unique combination of anxiety and ADHD symptoms made giving and asking for consent challenging. Previous research has discussed that, during adolescence, people with disabilities need to be taught what consent is and provided with strategies of helpful, accessible ways to ask for/give consent [ 44 ]. For Amie specifically, communicating about personal boundaries was uncomfortable during sexual scenarios:
[With my] combined anxiety and ADHD, I think there was a part of being scared to ask questions and then a part of not really being observant enough about, you know, like, I don't know, just not putting enough focus on the sex education that I did receive -the little sex education that I did receive … It's kind of depressing, but I feel, like, with my anxiety, I kind of struggle to speak up when maybe I didn't have any interest in a guy. Like if he's touching me or something [I don’t like] and like I just, like, run off or take off and not handle that in a correct way, where maybe somebody else would have [handled it differently] because they would have said, “Screw you!” or something like that and said I'm just like, “Oh God, what do I do?” Just, you know, not handling that correctly necessarily.
Gabrielle’s personal experiences with disability and interacting with others diverged from Amie and Alice’s experiences. She explained how, even though she was Deaf, having cochlear implants allowed her to “pass”, or appear more able-bodied, and hear more. And while passing did not directly affect her sexual experiences, Gabrielle explained how she came from a “socially open home” where her parents normalized talking to others about her Deafness:
When people asked me about it, I'm very like, you know, big on wanting to tell everything about it … I see myself as normal. If you were to put it- like not normal. But when you go out like yeah, like people are like they're like, Oh, you're deaf? Like I just got a new job on campus and my manager didn't know for like two weeks. Like I told him, he was like, "What!” Then I was like, “Yeah, I was like, I honestly just wanted to wait to see how long you'd have to figure that out. I thought you would have noticed.”
Influence of Media
Like the participants in the “self-guided journey,” various media platforms served as educational tools for relationships and dating for these participants as well. For Gabrielle, the media's influence was a continuation of socially learning from friends over an online platform. She also explained how shifts in societal messaging and cultural changes set the tone for the type of media she consumed:
[The media is] definitely more influential now like definitely since 2020 with all the queer and the LGBTQ awareness and all that, which I fully support. But like all that definitely makes a big difference with all sexuality and learning about that. Because now it's like education too. It's being a big influence on that as well because people are trying to figure out how to properly teach it without, you know, with [university] doing the whole pronoun thing. Now, that's a whole big deal. I feel like that's definitely a big change.
The influence of the media continued in Alice’s interview. She described how ‘smut books’ and porn taught her about personal grooming and sexual activities. Learning from the media was not always positive, though, as it enforced gendered stereotypes and contributed to her disordered eating.
I've watched a lot of different YouTubers or different people because people are getting more comfortable about the conversation topic and talk about what things to have, when things don't have, what things you think are good for it but are, and how to properly take care of yourself down there. So, I am very aware of that. And I'm trying to, I'm in a pretty good place, some pretty good rhythm with that now … I'd watched a ton of media. I read a lot of smut. It's what it's called, I guess, like smut books and stuff like that. I watched porn as well, which gave me kind of graphic yet unrealistic descriptions of what things would be like.
Whereas Gabrielle and Alice reflected on how media impacted the PHSE journey, Amie’s story did not include media influences. This was one way that her journey diverged from the others within the same story type.
Personal Health Matters More
The third story type, “Personal Health Matters More”, reflects the experiences of one participant, Cecelia. Compared to other participants and story types, Cecelia appeared to be in the beginning stages of her journey with PHSE. Romantic and sexual relationships with other people had not been priorities to Cecelia; in contrast, from a very young age, personal health was a top priority in her life. At seven years old, Cecelia was diagnosed with a brain tumor and grew up consciously trying to avoid comorbidities.
Sexual Information Was Not a Priority
Cecelia shared that she had not acquired sexual information. She described herself as not open or ready to learn about sexuality:
I feel like if I'm not open to be receptive to learning about it and it's not my top priority, then that's just where a disconnect could be in it. So, if I'm not ready to learn about it, then I just won't worry about it. So that's probably also why I just don't have so much information about it because I'm not asking questions either.
Not seeking out or being receptive to PHSE put Cecelia at the beginning of her PHSE journey. Where other story types presented narrative climaxes and turning points, Cecelia’s interview revealed that she was in the early stages of learning about PHSE. Her narrative truly showed how sexuality is not a linear experience where everyone develops at the same time and pace.
No School Sex Education
Her formal education in school settings included personal/general health, but not comprehensive sexual information.
Cecelia: We took like general health and high school, but more so focused on drugs, I guess, and alcohol usage within those classes. Interviewer: So, they didn't talk about like periods or pregnancies or safe sex? Cecelia: No. Not really.
Familial Support
Cecelia did report open communication with her mother and support with personal health goals from sisters. So, even though their conversations were not focused on topics like sexuality, Cecelia felt comfortable and open when communicating with her family members.
Interviewer: What about have you ever had those kinds of conversations with your family members? Cecelia: Kind of with my mom, I guess. Like I have, um, three other sisters. It's like they've talked about periods and stuff, but that's something that's part of one of my health issues is that I don't really get that, so I don't focus on that aspect of it. Then that's just about it. None of us have boyfriends, so our minds don't focus, right to like sex and safe sex techniques because that's not our main focus, I guess.
Her sisters were also not currently dating, so they were also not a source of direct or indirect learning about sexuality or romantic relationships. Cecelia’s sisters were, however, sources of “influence and encouragement” on her personal health.
I guess none of them have ever had a boyfriend. So, nothing really like dating wise. I guess like for my sisters, I've learned about the menstrual cycle and stuff and just because they get it. So, they've told me like, oh, this is what to expect or this, and that, that's what should be happening.
Prominence of Disability
Cecelia was diagnosed with a brain tumor in childhood and worried about comorbidities over the course of her life. Because of this awareness, she developed open communication with doctors and family members, and learned to advocate for herself in medical settings. Although her disability did not directly guide her sexual education experiences, it did influence her attention and care to learning about personal health.
So, I guess personal health started at a pretty young age just because when I was diagnosed with cancer, I was only seven. And so, prior to that, I had gone to doctors and like I struggled with weight problems. And so, I started to like, take control of my health then to try and combat gaining weight. And then later found out that I was diagnosed with cancer. And then I guess just from there, I started taking health into my own hands and trying to figure out, well how can I decrease the chances of getting other diseases and how can I better help myself overcome the disease I already had.
Two Ears, One Mouth
One participant experienced the final story type, which was named after an in-vivo code that explained his view on PHSE: “Two Ears, One Mouth”. Similar to “Personal Health Matters More”, the participant experiencing this final story type did not prioritize sexuality or dating even though there were supportive influences that provided PHSE knowledge, like family members and peers. However, contrary to “Personal Health Matters More”, “Two Ears, One Mouth” held themes of learning about sexuality and dating during adolescence. This story type also differed from “Experience is the Best Teacher” because formal and informal avenues of PHSE information provided Drew with enough accurate knowledge; however, he has not needed such information in his personal life. Instead, Drew prioritized his religion, well-being, and quality of life above romantic or sexual relationships.
[PHSE information] was a lot of in one ear out the other sort of a thing of like in a sense like denial, kind of like, “Okay, I've already heard this before, let’s move on” type of a thing… I'm definitely the person that I live by the model we have two ears and one mouth sort of a thing. So, listen before you speak.
Drew held confidence and satisfaction in the amount of PHSE he had acquired over time, but he has not had much need for it because dating and sexuality are not among his top priorities. He explained how he took in and adsorbed PHSE information during his adolescence. Internalized ableism and “special” treatment were also hallmarks to this story type that were not present in other participants’ journeys.
Dating and Sex Were Not Priorities
For Drew, dating and sexuality have not been top priorities. He acquired PHSE from multiple sources and had access to open conversations about things like puberty, dating, and sexuality; however, he did not seek out information or raise inquiries of his own.
I'm also very strong in my religious beliefs … So, I've kind of always prioritized that above everything and said, ‘I'm not even going to really- I take [relationships and sex] to heart’, but I'm also like- it's a little lesser priority over my religion and my religion is weighted anyway, that's going to hold the value over it … truthfully I'm just prioritizing myself.
Peers with Similar Priorities
Drew described his friend group as having the same priorities as him. This meant that they were not focusing on relationships and sex, and he was less prone to peer pressure because he was not presented with it.
I would say friends that share the similar viewpoint to me, of just like [dating and sex] is not super important, like we're not going to really engage in it anyway, like, to a good extent.
Positive, Supportive Family
Drew also described having open conversations with family members that equipped him with knowledge about dating and sexual activities. He felt comfortable in these conversations, but he was not the one seeking or applying the information.
I definitely had the at-home talk to like not just, you know sex-related. Just, you know, you should be or might be experiencing [puberty changes] and you can talk to us. One thing I will say about my family is that we are very close, very integrated, you know, we're a very tight knit family. So, my parents expressed from early on, you know, ‘Talk to us, we've all been through similar experiences that we all go through the same life development and all that. So, be free and willing to talk to us about whatever you're going through and we can help you out or we can reference you to something or whatever.’
Present, but Unhelpful, School Sex Education
The formal sex education that Drew received was fear-based or abstinence only. He reported not retaining much information though because it did not apply to his life.
Essentially, [teachers] say abstain, but obviously, that's somewhat unrealistic as you go farther and farther into life, they're like just be protected with it. You know, how to use condoms and all that and just kind of know consequences that could go with whatever you whatever actions you take. But then throughout middle school, I guess it was the same thing like you have just a certain education that I would say [is] very similar to elementary school… And how to protect yourself against STD or STI and all that sort of thing. And again, I would say like, I've internalized that a little bit more but it was still like a, ‘Alright, this isn't going to pertain to me for a little bit’. My personal opinion [schools] don't teach it well. They definitely undervalue [sex education] and they can do a better job at it. But they do teach it.
Drew’s narrative held the most prominent examples of internalized ableism, which affected his overall educational experiences, although he did not specifically describe whether it affected his PHSE. At first, he described how prominent his impaired hearing was during his childhood because his hearing aids were visible and he had additional support in instructional settings. He described receiving special treatment and being coddled by educators, family, and peers.
Especially when I was young, I would definitely say I had a special treatment like all throughout elementary and I would say especially as I got to like middle school…I did have a hearing aid and all of that, especially up until like seventh grade at least. And not only that, but throughout elementary school my teachers would have some sort of necklace/microphone I guess, but it was like a very fancy necklace [with a microphone]. So, when they spoke, it literally went directly in my ear like somebody would just be talking at a normal volume… It was basically to the point where like all my classmates knew about it. Like all my classmates knew that it kind of pointed me out to everyone. I was never bullied or anything, like, I never had that negative treatment, but it definitely made it to where everyone was like, “Alright, he has that. He's the kid [who can’t hear]” sort of a thing. And I would definitely say that it impacted a little bit of just how some people treated me, like, again no one ever bullied me or anything. But they always kind of, I guess, even outside of the house, [everyone] coddled me.
Although he did not describe it affecting his sexuality development or education, internalized ableism influenced how Drew presented himself as he transitioned between grade levels. By high school, in an attempt to “pass” amongst his peers, Drew wore his hearing aids less often.
Looking back at it, I'll be completely honest with you, I never thought about this until actually just sharing this [in the interview]. But looking back at it, that might be the reason why when I went to high school, I just ditched my hearing aids. I didn’t want to stand out. I just wanted to fit in and conform. I kind of said to myself I would rather deal with only hearing 75% of the conversation and not standing out than having this advantage of hearing [like everyone else] ... I was known as the person that had the hearing aid and I internalized the standing out sort of a thing.
The Absence of Sexuality and Disability Interaction
Finally, the absence of sexuality and disability intersections in Drew’s narrative became apparent in data analysis. Although Drew explained his disabilities and how they affected his life and some experiences, he did not describe any time when his disabilities affected intimate or sexual interactions with others. Teachers, family members, and peers did not change the way they interacted with him due to his symptoms or diagnoses. Having no interaction between sexuality and disability symptoms may have been due to the deprioritization of sexual relationships and Drew’s ability to “pass”, similar to how Gabrielle passed while using cochlear implants in the second story type, “Experience is the Best Teacher”.
The findings from this study provide a glimpse of possible ways individuals growing up with disabilities learn about personal health and sexuality. Participants’ experiences showed that, as is common in general populations (e.g., [ 13 ]), formal sources of PHSE information such as schools and medical providers did not provide accurate or adequate PHSE. When formal educators proved unhelpful and unsupportive, individuals looked toward informal support from family members, peers, and media. An added challenge for individuals growing up with disabilities was discovering how their unique symptoms interacted with their sexuality development. Disability symptoms played a role in individuals’ sexuality development and intimate experiences with others. This study illustrates how varied disability characteristics inform young adults’ journeys seeking PHSE information and expand on current research of sexuality and disability by giving further insight to diverse experiences of sexuality development of disabled adolescents.
Formal and Informal Sources of PHSE
Our findings show similarities between the PHSE experiences of people with disabilities and the general population. Unfortunately, exposure to poor or nonexistent sex education in schools, uninformed medical providers, and uncomfortable conversations with family members about sex are common experiences among youth [ 13 ]. Participants in this sample had the added challenge of finding helpful and informed educators who could advise on the interaction of their sexuality development and specific disability symptoms.
Some participants described not having received PHSE in schools. When they did receive sex education, it was fear-based, largely focused on abstinence, and not inclusive. Similar to our findings, in a longitudinal study from 2015 to 2019 in the United States, researchers found that 53% of female adolescents and 54% of male adolescents had received sexual education, and, of those who received sexual education, 81% of female adolescents and 79% of male adolescents reported specifically receiving “say no to sex” (abstinence-based) education [ 26 ]. All of our participants expressed a desire for more universal, comprehensive PHSE from schools, which is consistent with previous research that found that adolescents want PHSE education that is focused on comprehensive sexuality [ 18 ].
Having diagnosed disabilities adds an extra layer of context around PHSE experiences because there are other formal supports that provide health information specific to symptoms, like medical providers. Doctors and other medical providers were another formal way that individuals’ sexuality, development, and disabilities intersected. When participants had a more open dialogue with their doctors, they were more likely to ask questions and communicate about their disabilities and sexuality. Some participants described receiving inaccurate information from doctors and experiencing judgmental interactions with medical providers, which was particularly important to individuals who told “The Self-Guided Journey” narrative. These findings were consistent with previous research that explains how difficult finding a well-trained, understanding medical professional can be for the disabled population [ 5 ].
For the individuals who experienced inadequate PHSE information from authority figures, like schools and medical providers, informal educators held great influence. Family members appeared in every story type, whether it was as helpful supporters or unhelpful, inadequate resources. Regardless of ability status, previous research has shown that family members, especially parents, do not always know how to talk about sexuality development [ 35 ]. This was apparent in multiple stories as some parents indirectly discussed sexuality or actively avoided sexual discussions. A lack of useful and accessible materials for informal PHSE that caregivers and families can provide disabled loved ones with is a barrier to PHSE for disabled communities. Even though literature with guides, advice, and practices about teaching PHSE exists for families of youth with disabilities [ 10 , 17 , 19 , 48 , 49 ], we hypothesize that such resources are not being used by caregivers because they are not disseminated widely from providers and are not entirely accessible. Our findings also showed the influence of siblings when it comes to learning about personal health and sexuality. Consistent with previous literature [ 35 , 36 ], participants’ siblings were supportive, positive resources for sexual information and sexuality development conversations.
Many participants learned about sexuality and the role of their disabilities in their sexuality from the media. Our findings add to past research that has begun to describe how media such as television, websites, and social media can be important educational tools for adolescents and young adults with disabilities during their sexuality development [ 1 , 11 , 12 , 20 , 31 ]. Our participants described media avenues to learning about personal health and sexuality development like reading books and pamphlets, using the internet to access pornography, and joining online organizations for people with their shared disabilities and symptoms. Our findings indicate that media remain important for people with disabilities and are influences in young people’s lives.
Sexuality Development in the Context of Disability
Our findings highlight diversity within the lived experiences of emerging adults with disabilities, adding nuance to understanding of sexuality development. While some participants were ready to receive PHSE information in adolescence, others were not. Journeys to acquiring PHSE information were not linear nor did they follow a progressive developmental path. Contrary to prior research that suggests differences in timing of sexual experiences may not be significant for people with disabilities [ 11 , 12 ], our findings clearly show how disability symptoms can influence the timing of readiness to receive PHSE. For example, Brandy’s Crohn’s disease delayed her puberty. Other participants, like Drew and Cecelia, were focused on their health and not their sexual or romantic relationships when they received formal PHSE. Individuals’ disabilities informed their developmental journeys. Even if adolescents with disabilities receive comprehensive PHSE that is relevant to their needs, that education will not be helpful if they are not developmentally at the point where such information would be applicable. Therefore, simply providing PHSE during adolescence is not enough – the timing of when it would be most appropriate must be considered as well.
Furthermore, where disability came into all participants’ PHSE stories—and where it did not—suggested the extent to which participants perceived their disability interacting with their lives. For example, the three participants who told a Self-Guided Journey had clear reflections on how their symptoms and diagnoses affected their sexuality development and the way others interacted with them. Their PHSE stories included disability reflections from start to finish. This was not the case for all of the participants, though. When reflections on the intersection of disability symptoms and sexuality came near the end of participants’ stories, it was more in response to probing questions rather than spontaneous as participants had not thought about the connections before. For example, in “Experience is the Best Teacher”, Amie began the interview by sharing her story and experiences learning about sexuality, and only started tying her ADHD symptoms to sexual experiences near the end of the interview when she realized that her experiences were intertwined with her symptoms. When reflections of the intersection between disability and sexuality development were not as present until the end of participants’ stories, it was clear that they did not originally consider their disability as a central part of their PHSE journey. Although some disability symptoms have more impact on a person’s life, diagnoses are only a piece of an individual’s experience and interact with every part of who they are—including how they develop sexually and interact with others. Our findings add to the current literature that emphasizes diversity in disabilities and experiences with sexuality [ 5 , 39 ]. Specifically, our findings demonstrate how disability symptoms and personal characteristics impact individuals’ sexuality development in different ways even when participants were in a similar age range and stage of life.
Social Policy Implications
Linearity in sexuality development should not be expected, nor should it be expected that people at the same age are in the same stage of sexuality development. Our participants expressed how unhelpful some of their PHSE was due to poor timing; school-based PHSE was not relevant to them at the time they received it because they were not physically and/or emotionally ready for sexual relationships. Therefore, sexual education in formal settings should not assume someone’s readiness to receive PHSE information. A universally designed sexual education would be most beneficial to adolescents, regardless of ability status. Universal design principles have been applied in sexuality surveys and research for disabled individuals [ 66 ], though this research area is not expansive and needs further exploration. Our findings reinforce the need for more universally designed PHSE programs. A universally designed PHSE curriculum would provide everyone with accessible, helpful PHSE. Universally designed PHSE would include instruction about varied abilities and would empower individuals to learn at their own pace a wealth of sexual information that pertains to both the general population and their specific needs. The next step for researchers should be gathering ample amounts of information on the sexuality-related needs, desires, and lived experiences of people who grew up with or acquired disabilities, and then distributing accessible and helpful information to supporters and resources for all disabled communities.
Individualization within disabilities and disability presentation exists. Medical providers, especially those providing diagnoses, need to have more PHSE information for individuals with disabilities and recognize that a one-size-fits-all model is unrealistic and not helpful. Research has shown that medical providers have mixed comfort levels and little knowledge about the sexuality of people living with disabilities [ 11 , 12 , 32 , 57 ]. To fix this problem for medical providers and patients, providers who interact with disabled communities should educate themselves on the sexual experiences of disabled people by listening to the voices of this community. There should not be an assumption that children with disabilities are asexual or that they develop at the same time as every other child.
Finally, the internet has the potential to help or harm young people depending on the reliability of web pages and content creators. So long as the information on web pages is accurate and developmentally appropriate, the internet can aid in teaching children and adolescents PHSE that is more tailored to their individual needs, like disability symptoms and personal readiness [ 53 ]. However, young people are also vulnerable to experiencing negative consequences of online exploration, such as cyber-sexual violence victimization and inaccurate PHSE information [ 61 ]. Experiences with cyber-sexual violence victimization and pornography use in adolescence can be associated with risky sexual behaviors, like lack of condom use, birth control use, and substance use [ 53 ]. Guardians, parents, and influential adults also have opportunities to involve themselves in media consumption, through parental monitoring and open conversations, which can support healthy adolescent sexuality development [ 53 ].
Limitations
As with any research study, this study held some limitations. The sample was mostly white (87.5%) and composed of women (75%). Qualitative narrative analysis traditionally has smaller sample sizes in order to preserve the nuances of participants’ stories and not generalize experiences [ 33 ]. However, since this study had eight participants, it did not capture all possible experiences of learning about PHSE of individuals growing up with disabilities. Additionally, all of the participants experienced mainstream schooling, which meant there were no experiences shared from individuals that went through Special Education programs in public schools or home-schooling. We also had no participants with intellectual disabilities. Since non-mainstream students experience different classroom settings and lecture content, their experiences learning about personal health and sexuality are likely to have a different set of complexities compared to those in our sample [ 40 , 63 ]. Individuals with intellectual disabilities also have unique needs from PHSE [ 30 , 40 , 54 ]. Future researchers should strive to capture additional PHSE narratives from a more diverse sample of individuals with disabilities.
Emerging adults with disabilities were not represented in classroom PHSE, but they experienced agency in seeking out information from additional sources such as media and families. Although our findings presented individuals’ agency in seeking out and acquiring helpful PHSE information, it should not be left to the individual—especially during childhood or adolescence—to educate themselves on sexuality and health related topics. Young people growing up with (and without) disabilities need to have helpful educators from multiple outlets, like families, medical providers, peers, schools, etc. Inclusive design for sexual education is not only an issue for people with disabilities and, if implemented across the United States, would greatly benefit younger generations’ sexual knowledge.
Data Availability
Data collection was approved by the Institutional Review Board at Virginia Polytechnic Institute and University. Data was analyzed using MAXQDA.
The terms “disabled people” and “people with disabilities” will be used interchangeably [ 15 ] throughout this study. This word usage is intentional as different disabled communities use each terminology, and the study seeks to capture disability as its own category rather than separating each condition or experience. It is important to acknowledge that the author understands that this terminology is an individual’s choice,by using both identifying phrases, it is my hope to represent as much of the disabled community as possible. Furthermore, in this paper, I use the official federal/legal definition of disability: “An individual with a disability is defined by the ADA as a person who has a physical or mental impairment that substantially limits one or more major life activities, a person who has a history or record of such an impairment, or a person who is perceived by others as having such an impairment” [ 2 ].
Ahrens, J., Upper, R., Loh, E., Wolfe, D., Giurleo, C., Courten, E., Mehta, S.: Internet-based sexual health resources for those living with spinal cord injury: a content analysis. J. Spinal Cord Med. (2023). https://doi.org/10.1080/10790268.2023.2220509
Article PubMed PubMed Central Google Scholar
Americans With Disabilities Act Amendment Act of 2008, Pub. L. No. 110-325, 42 USCA. 12101 note (2008)
Alexander, N., Taylor Gomez, M.: Pleasure, sex, prohibition, intellectual disability, and dangerous ideas. Reprod. Health Matter. 25 (50), 114–120 (2017). https://doi.org/10.1080/09688080.2017.1331690
Article Google Scholar
Awaru, A. O. T., Torro, S., Agustang, A. D. M. P., Nurmaidah, A.: Sexual education of children with down syndrome in parents low education. In 3rd International Conference on Social Sciences (ICSS 2020) (pp. 524–529). Atlantis Press (2020). https://doi.org/10.2991/assehr.k.201014.115
Barbareschi, G., Wu, Z.: Accessing intimate interactions: Investigating the need for more inclusive sex education resources. In CHI Conference on Human Factors in Computing Systems Extended Abstracts (pp. 1–6). (2022, April). https://doi.org/10.1145/3491101.3519747
Basile, K.C., Breiding, M.J., Smith, S.G.: Disability and risk of recent sexual violence in the United States. Am. J. Public Health 106 (5), 928–933 (2016). https://doi.org/10.2105/AJPH.2015.303004
Brown, J., Patrician, P.A., Shirey, M.R., Ladores, S.: Sexual and reproductive health in women with cystic fibrosis: a dimensional concept analysis. J. Nurs. Pract. Appl. Rev. Res. 6 (7), 5–12 (2019)
Google Scholar
Burchardt, T.: Capabilities and disability: the capabilities framework and the social model of disability. Disabil. Soc. 19 (7), 735–751 (2004). https://doi.org/10.1080/0968759042000284213
Campbell, M.: Disabilities and sexual expression: a review of the literature. Sociol. Compass 11 (9), e12508 (2017). https://doi.org/10.1111/soc4.12508
Couwenhoven, T.: Teaching Children with Down Syndrome About Their Bodies, Boundaries, and Sexuality: A Guide for Parents and Professionals. Woodbine House (2007)
Crehan, E.T., Rocha, J., Sclar, J., Ward, O., Donaghue, A.: Topics and timing of sexuality and relationship education for autistic and non-autistic adults in the United States. Disabil. Health J. 16 (3), 101466 (2023). https://doi.org/10.1016/j.dhjo.2023.101466
Article PubMed Google Scholar
Crehan, E.T., Schwartz, A.E., Schmidt, E.K.: Who is delivering sexual health education content to young adults with intellectual or developmental disability?: A survey of us-based school-based professionals and parents. Sex. Disabil.Disabil. (2023). https://doi.org/10.1007/s11195-023-09790-2
Davies, A.W., Bryan, M.K., Martin, T., Shay, B., Akers, T., Soud, R., Neustifter, R.: Dismantling barriers to access: the necessity of cripping sexuality education in Canadian schools. Can. J. Hum. Sex. 32 (1), 1–19 (2023). https://doi.org/10.3138/cjhs.2022-0031
Dewinter, J., Vermeiren, R., Vanwesenbeeck, I., Van Nieuwenhuizen, C.: Autism and normative sexual development: a narrative review. J. Clin. Nurs. 22 (23–24), 3467–3483 (2013). https://doi.org/10.1111/jocn.12397
Dwyer, P.: Stigma, incommensurability, or both? Pathology-first, person-first, and identity-first language and the challenges of discourse in divided autism communities. J. Dev. Behav. Pediatr. 43 (2), 111–113 (2022). https://doi.org/10.1097/DBP.0000000000001054
Etherington, C., Huntington, S., Conway, S.P., Peckham, D.: 294 Survey of contraceptive practices in women attending a large regional UK centre. J. Cyst. Fibros. 11 , S132 (2012). https://doi.org/10.1016/s1569-1993(12)60462-7
Fogel, L.: Partnering clinician-and parent-led organizations for guidance on puberty and menarche in cerebral palsy and intellectual disability. Dev. Med. Child Neurol. 63 (2), 128–128 (2021). https://doi.org/10.1111/dmcn.14728
Formby, E., Donovan, C.: Sex and relationships education for LGBT+ young people: Lessons from UK youth work. Sexualities 23 (7), 1155–1178 (2020). https://doi.org/10.1177/1363460719888432
Frank, K., Sandman, L.: Supporting parents as sexuality educators for individuals with intellectual disability: the development of the home BASE curriculum. Sex. Disabil. 37 (3), 329–337 (2019). https://doi.org/10.1007/s11195-019-09582-7
Friedman, C., Arnold, C.K., Owen, A.L., Sandman, L.: Remember our voices are our tools: sexual self-advocacy as defined by people with intellectual and developmental disabilities. Sex. Disabil. 32 , 515–532 (2014). https://doi.org/10.1007/s11195-014-9377-1
Frayman, K.B., Sawyer, S.M.: Sexual and reproductive health in cystic fibrosis: a life-course perspective. Lancet Respir. Med. 3 (1), 70–86 (2015). https://doi.org/10.1016/S2213-2600(14)70231-0
Gokgoz, C., Demirci, A. D., Kabukcuoglu, K.: Sexual behaviours and education in adolescents and young adults with Down syndrome: A grounded theory study of experiences and opinions of their mothers in Turkey. Res. Dev. Disabil. 112 , 103907 (2021)
Gokgoz, C., Demirci, A. D., & Kabukcuoglu, K. Sexual behaviours and education in adolescents and young adults with Down syndrome: A grounded theory study of experiences and opinions of their mothers in Turkey. Res. Dev. Disabil. 112 , 103907 (2021). https://doi.org/10.1016/j.ridd.2021.103907
Gray, S.H., Wylie, M., Christensen, S., Khan, A., Williams, D., Glader, L.: Puberty and menarche in young females with cerebral palsy and intellectual disability: a qualitative study of caregivers’ experiences. Dev. Med. Child Neurol. 63 (2), 190–195 (2021). https://doi.org/10.1111/dmcn.14698
Greenwood, N.W., Wilkinson, J.: Sexual and reproductive health care for women with intellectual disabilities: A primary care perspective. Int. J. Fam. Med. 2013 , 642647 (2013). https://doi.org/10.1155/2013/642472
Guttmacher Institute. US adolescents’ receipt of formal sex education. Guttmacher Institute. (2022, February). https://www.guttmacher.org/fact-sheet/adolescents-teens-receipt-sex-education-united-states
Harrell, E. Crime against persons with disabilities, 2009–2015-Statistical tables. Bureau of Justice Statistics. (2017). https://bjs.ojp.gov/content/pub/pdf/capd0915st.pdf
Hartley, S., Muhit, M.: Using qualitative research methods for disability research in majority world countries. Asia Pac. Disabil. Rehabil. J. 14 (2), 103–114 (2003)
Havermans, T., Abbott, J., Colpaert, K., De-Boeck, K.: Communication of information about reproductive and sexual health in cystic fibrosisPatients, parents and caregivers’ experience. J. Cystic Fibrosis 10 (4), 221–227 (2011). https://doi.org/10.1016/j.jcf.2011.04.001
Hayashi, M., Arakida, M., Ohashi, K.: The effectiveness of a sex education program facilitating social skills for people with intellectual disability in Japan. J. Intellect. Dev. Disabil. 36 (1), 11–19 (2011). https://doi.org/10.3109/13668250.2010.549463
Hole, R., Schnellert, L., Cantle, G.: Sex: What is the big deal? Exploring individuals’ with intellectual disabilities experiences with sex education. Qual. Health Res. 32 (3), 453–464 (2022). https://doi.org/10.1177/10497323211057090
Holmes, L.G., Himle, M.B., Sewell, K.K., Carbone, P.S., Strassberg, D.S., Murphy, N.A.: Addressing sexuality in youth with autism spectrum disorders: current pediatric practices and barriers. J. Dev. Behav. Pediatr. 35 (3), 172–178 (2014). https://doi.org/10.1097/DBP.0000000000000030
Josselson, R., Hammack, P.L.: Essentials of Narrative Analysis. American Psychological Association (2021)
Book Google Scholar
Jun, H.: Disablism/Ableism. In: Jun, H. (ed.) Social justice, multicultural counseling, and practice, pp. 243–271. Springer, Cham (2018)
Chapter Google Scholar
Kaestle, C.E., Allen, K.R., Wesche, R., Grafsky, E.L.: Adolescent sexual development: a family perspective. J. Sex Res. 58 (7), 874–890 (2021). https://doi.org/10.1080/00224499.2021.1924605
Killoren, S.E., Roach, A.L.: Sibling conversations about dating and sexuality: sisters as confidants, sources of support, and mentors. Fam. Relat. 63 (2), 232–243 (2014). https://doi.org/10.1111/fare.12057
Kitchin, R.: The researched opinions on research: disabled people and disability research. Disabil. Soc. 15 (1), 25–47 (2000). https://doi.org/10.1080/09687590025757
Klebanov, B., Friedman-Hauser, G., Lusky-Weisrose, E., Katz, C.: Sexual abuse of children with disabilities: key lessons and future directions based on a scoping review. Trauma Violence Abuse (2023). https://doi.org/10.1177/15248380231179122
Loeser, C., Pini, B., Crowley, V.: Disability and sexuality: desires and pleasures. Sexualities 21 (3), 255–270 (2018). https://doi.org/10.1177/1363460716688682
Löfgren-Mårtenson, L.: “I want to do it right!” a pilot study of Swedish sex education and young people with intellectual disabilities. Sex. Disabil. 30 (2), 209–225 (2012). https://doi.org/10.1007/s11195-011-9239-z
Mabusi, M., Kivuma, B.: Assessment of knowledge, perception, and practice on sexual and reproductive health among adolescents with disabilities at Ilala, Dar Es Salaam. AIJR Abstracts, 26. (2021). https://books.aijr.org/index.php/press/catalog/book/116/chapter/1165
Mailhot Amborski, A., Bussieres, E.L., Vaillancourt-Morel, M.P., Joyal, C.C.: Sexual violence against persons with disabilities: a meta-analysis. Trauma Violence Abuse 23 (4), 1330–1343 (2022). https://doi.org/10.1177/1524838021995975
Marques Bononi, B., Carvalho Sant'Anna, M., Chao Vasconcellos de Oliveira, A., Silveira Renattini, T., Franchi Pinto, C., Passarelli, M., Coates, V., Omar, H.: Sexuality and persons with Down syndrome. A study from Brazil. Int. J. Adolesc. Med. Health 21 (3), 319–326 (2009). https://doi.org/10.1515/IJAMH.2009.21.3.319
McCarthy, M., Thompson, D.: A prevalence study of sexual abuse of adults with intellectual disabilities referred for sex education. J. Appl. Res. Intellect. Disabil. 10 (2), 105–124 (1997). https://doi.org/10.1111/j.1468-3148.1997.tb00012.x
McRuer, R.: Crip theory: Cultural Signs of Queerness and Disability. NYU Press (2006)
McRuer, R.: Disabling sex: notes for a crip theory of sexuality. GLQ A J. Lesbian Gay Stud. 17 (1), 107–117 (2011). https://doi.org/10.1215/10642684-2010-021
Michielsen, K., Brockschmidt, L.: Barriers to sexuality education for children and young people with disabilities in the WHO European region: a scoping review. Sex Educ. 21 (6), 674–692 (2021). https://doi.org/10.1080/14681811.2020.1851181
Nichols, S., Moravcik, G.M., Tetenbaum, S.P.: Girls Growing Up on the Autism Spectrum: What Parents and Professionals Should Know About the Pre-Teen and Teenage Years. Jessica Kingsley Publishers (2009)
Phelps, R.A.: Teaching children with down syndrome about their bodies, boundaries, and sexuality: a guide for parents and professionals. J. Dev. Behav. Pediatr. (2009). https://doi.org/10.1097/01.DBP.0000359325.34945.06
Pyer, M., Campbell, J.: Qualitative researching with vulnerable groups. Int. J. Ther. Rehabil.Ther. Rehabil. 19 (6), 311–316 (2012)
Riessman, C.K.: Narrative methods for the human sciences. Sage (2008)
Rioux, M.H.: Bending Towards Justice. In: Barton, L. (ed.) Disability, Politics and the Struggle for Change, pp. 34–48. David Fulton (2001)
Rivas-Koehl, M., Valido, A., Espelage, D.L., Lawrence, T.I.: Adults and family as supportive of adolescent sexual development in the age of smartphones? Exploring cybersexual violence victimization, pornography use, and risky sexual behaviors. Arch. Sex. Behav.Behav. (2023). https://doi.org/10.1007/s10508-023-02618-2
Schaafsma, D., Kok, G., Stoffelen, J.M., Curfs, L.M.: Identifying effective methods for teaching sex education to individuals with intellectual disabilities: a systematic review. J. Sex Res. 52 (4), 412–432 (2015). https://doi.org/10.1080/00224499.2014.919373
Scholars Strategy Network. (2019, October 10). Why sex education in the United States needs an update and how to do it. Scholars Strategy Network. https://scholars.org/contribution/why-sex-education-united-states-needs-update-and-how-do-it
Shakespeare, T.: The Social Model of Disability. In: Davis, L.J. (ed.) The Disability Studies Reader, 2nd edn., pp. 197–204. Taylor & Francis (2006)
Shindel, A.W., Ando, K.A., Nelson, C.J., Breyer, B.N., Lue, T.F., Smith, J.F.: Medical student sexuality: how sexual experience and sexuality training impact US and Canadian medical students’ comfort in dealing with patients’ sexuality in clinical practice. Acad. Med. J. Assoc. Am. Med. Col. 85 (8), 1321 (2010). https://doi.org/10.1097/ACM.0b013e3181e6c4a0
Shivayogi, P.: Vulnerable population and methods for their safeguard. Perspect. Clin. Res. 4 (1), 53 (2013). https://doi.org/10.4103/2229-3485.106389
Smith-Chandler, N., Swart, E.: In their own voices: methodological considerations in narrative disability research. Qual. Health Res. 24 (3), 420–430 (2014). https://doi.org/10.1177/1049732314523841
Stafford, L.: ‘What about my voice’: Emancipating the voices of children with disabilities through participant-centred methods. Children’s Geogr. 15 (5), 600–613 (2017). https://doi.org/10.1080/14733285.2017.1295134
Stoilova, M., Livingstone, S., Khazbak, R.: Investigating risks and opportunities for children in a digital world: a rapid review of the evidence on children’s internet use and outcomes. Unicef (2021)
Tolman, D.L., McClelland, S.I.: Normative sexuality development in adolescence: a decade in review, 2000–2009. J. Res. Adolesc. 21 (1), 242–255 (2011). https://doi.org/10.1111/j.1532-7795.2010.00726.x
Treacy, A.C., Taylor, S.S., Abernathy, T.V.: Sexual health education for individuals with disabilities: a call to action. Am. J. Sex. Educ. 13 (1), 65–93 (2018). https://doi.org/10.1080/15546128.2017.1399492
Turner, G.W., Crane, B.: Sexually silenced no more, adults with learning disabilities speak up: a call to action for social work to frame sexual voice as a social justice issue. Br. J. Soc. Work. 46 (8), 2300–2317 (2016). https://doi.org/10.1093/bjsw/bcw133
Vlachou, A.: Education and inclusive policy-making: Implications for research and practice. Int. J. Incl. Educ. 8 (1), 3–21 (2004). https://doi.org/10.1080/1360311032000139449
Wilds, K. A. The hidden curriculum of dating: Creating a sexuality interests and sources of information survey for students with intellectual and developmental disabilities in inclusive post-secondary education. (2022). Retrieved from http://login.ezproxy.lib.vt.edu/login?url=https://www.proquest.com/dissertations-theses/hidden-curriculum-dating-creating-sexuality/docview/2730796304/se-2
Download references
This study did not receive outside funding from any organizations.
Author information
Authors and affiliations.
Department of Human Development and Family Science, Virginia Polytechnic Institute and State University, 248 Wallace Hall, 295 West Campus Drive, Blacksburg, VA, 24061, USA
Madelyn Toman & Rose Wesche
Department of Psychology, Niagara University, 102B DePaul Hall, New York, NY, 14109, USA
Carolyn M. Shivers
You can also search for this author in PubMed Google Scholar
Contributions
All authors agree to the content of the study and authorship order.
Corresponding author
Correspondence to Madelyn Toman .
Ethics declarations
Conflict of interest.
The authors have no conflicts to report.
Informed Consent
Informed consent was contained from all individuals included in this study.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Toman, M., Wesche, R. & Shivers, C.M. Narratives of Personal Health and Sexual Education Experiences of Emerging Adults with Disabilities. Sex Disabil (2024). https://doi.org/10.1007/s11195-024-09870-x
Download citation
Accepted : 23 August 2024
Published : 02 September 2024
DOI : https://doi.org/10.1007/s11195-024-09870-x
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Disabilities
- Sexual education
- Crip theory of sexuality
- Qualitative
- United States
- Find a journal
- Publish with us
- Track your research
IMAGES
VIDEO
COMMENTS
There are several types of interviews, often differentiated by their level of structure. Structured interviews have predetermined questions asked in a predetermined order. Unstructured interviews are more free-flowing. Semi-structured interviews fall in between. Interviews are commonly used in market research, social science, and ethnographic ...
Vancouver, Canada. Abstract. Interviews are one of the most promising ways of collecting qualitative data throug h establishment of a. communication between r esearcher and the interviewee. Re ...
Introduction. Interviewing people is at the heart of qualitative research. It is not merely a way to collect data but an intrinsically rewarding activity—an interaction between two people that holds the potential for greater understanding and interpersonal development. Unlike many of our daily interactions with others that are fairly shallow ...
Develop an interview guide. Introduce yourself and explain the aim of the interview. Devise your questions so interviewees can help answer your research question. Have a sequence to your questions / topics by grouping them in themes. Make sure you can easily move back and forth between questions / topics. Make sure your questions are clear and ...
Here are some steps on how to analyze a qualitative interview: 1. Transcription. The first step is transcribing the interview into text format to have a written record of the conversation. This step is essential to ensure that you can refer back to the interview data and identify the important aspects of the interview.
University Writing & Speaking Center. 1664 N. Virginia Street, Reno, NV 89557. William N. Pennington Student Achievement Center, Mailstop: 0213. [email protected]. (775) 784-6030. Using an interview can be an effective primary source for some papers and research projects.
5. Not keeping your golden thread front of mind. We touched on this a little earlier, but it is a key point that should be central to your entire research process. You don't want to end up with pages and pages of data after conducting your interviews and realize that it is not useful to your research aims.
InterViews by Steinar Kvale Interviewing is an essential tool in qualitative research and this introduction to interviewing outlines both the theoretical underpinnings and the practical aspects of the process. After examining the role of the interview in the research process, Steinar Kvale considers some of the key philosophical issues relating ...
In this article I discuss whether asynchronous written online interviews (e.g., via e-mail or a web forum) can be conducted narratively and based on guidelines, or whether the potential of written interviews is only reserved for certain forms of qualitative procedures. ... Written Online Interviews in Qualitative Social Research: On the ...
6.1 Interviews. In-depth interviews allow participants to describe experiences in their own words (a primary strength of the interview format). Strong in-depth interviews will include many open-ended questions that allow participants to respond in their own words, share new ideas, and lead the conversation in different directions. The purpose of open-ended questions and in-depth interviews is ...
Including interviews in your dissertation. To present interviews in a dissertation, you first need to transcribe your interviews. You can use transcription software for this. You can then add the written interviews to the appendix. If you have many or long interviews that make the appendix extremely long, the appendix (after consultation with ...
What are interviews? An interviewing method is the most commonly used data collection technique in qualitative research. 1 The purpose of an interview is to explore the experiences, understandings, opinions and motivations of research participants. 2 Interviews are conducted one-on-one with the researcher and the participant. Interviews are most appropriate when seeking to understand a ...
Revised on June 22, 2023. A structured interview is a data collection method that relies on asking questions in a set order to collect data on a topic. It is one of four types of interviews. In research, structured interviews are often quantitative in nature. They can also be used in qualitative research if the questions are open-ended, but ...
10. Be willing to make "on the spot" revisions to your interview protocol. Many times when you are conducting interviews a follow up question may pop into your mind. If a question occurs to you in the interview ask it. Sometimes the "ah-ha" question that makes a great project comes to you in the moment.
3. People's espoused theories differ from their theories-in-practice. Get them to tell a story. Ask "how" questions not "do". Use "tell me about" and "tell me more about that". Use open-ended questions. Approach your topic sideways. Don't take the first answer as a final answer. Ask for elaboration.
A qualitative research interview is a one-to-one data collection session between a researcher and a participant. Interviews may be carried out face-to-face, over the phone or via video call using a service like Skype or Zoom. There are three main types of qualitative research interview - structured, unstructured or semi-structured.
Before You Write. Of course, before you can incorporate interview data into your writing, you need to plan and conduct your interviews and begin to analyze your findings. Interviewing is a common form of research and information gathering in many different fields and across many different genres.
result, the structure of interviews can range from loose conversations to structured exchanges in which all interviewees are asked the exact same set of questions. Your choice of interview structure should reflect the goals and stage of your research. Less structured interviews are most appropriate for early stages of research because they
Writing interview questions. Harvard's Department of Sociology provides some steps to help guide you in the process of writing interview questions (see the link to the guide below). Write down the larger research questions of the study. Outline the broad areas of knowledge that are relevant to answering these questions.
As no research interview lacks structure most of the qualitative research interviews are either semi-structured, lightly structured or in-depth. ... Hand written notes during the interview are relatively unreliable, and the researcher might miss some key points. The recording of the interview makes it easier for the researcher to focus on the ...
Figure 9.2 provides an example of an interview guide that uses questions rather than topics. Figure 9.2 Interview guide displaying questions rather than topics. As you might have guessed, interview guides do not appear out of thin air. They are the result of thoughtful and careful work on the part of a researcher.
This article, aimed at the novice researcher, is written to address the increased need to develop research protocols or interview guides to meet the requirements set by IRBs and human subjects ...
5. Be honest. If your written interview involves responding to a series of questions about your skills, qualifications or opinions about aspects of the role, always answer them honestly. This interview process should help both you and your potential employers assess whether this is the right fit.
This article explores the relationships between the American health-care system, trust in institutions, and decision-making processes that have affected COVID-19 vaccine uptake. Findings are based on an analysis of a nationally representative sample of 137 individuals who participated in semi-structured qualitative interviews during the rollout of the first publicly available vaccine in the ...
Interview research tip number three, use the Evolve Career Library to get access to exclusive reports and reviews on your target company. This tip is mainly for college students because most universities have access to vault.com's premium databases, and that premium content is a main differentiator between vault.com and free websites like ...
This research explores the potential of large language models (LLMs) in revolutionizing report-writing practices across the criminal justice system. Drawing on insights from 23 interviews with justice professionals regarding report writing and LLM utilization, the benefits, challenges, and implications of integrating artificial intelligence (AI ...
Teacher educators struggle to balance heavy teaching loads, research, writing, and institutional service. This qualitative study uses institutional ethnography to question how college leadership understand the significance of academic scholarship in the professional lives of college-based teacher educators in Israel. Data from interviews with eight college position holders shed light on the ...
Individuals with varied disabilities were intentionally included to add breadth to the research field. The final sample consisted of eight individuals (75% female, 87% White, mean age of 21.5). After conducting narrative interviews and analyses, four story types were generated: (1) "The Self-Guided Journey", (2) "Experience is the Best ...
Written by Sheryl Sheth for TipRanks -> In our previous article on Immunic (IMUX) , we highlighted some of the important insights from the interview hosted by TipRanks with the company's ...